Less medicalese, please
Editor's note: Kevin Fulmer is senior manager client services at Verilogue, a Horsham, Pa., research firm.
Each year, over one billion conversations occur between health care providers and patients within the United States. If the collective goals of the health care industry are to enhance care, reduce cost and improve patient outcomes, we must go beyond researching patients and health care providers in isolation and acquire a deep understanding of the dynamics, challenges and opportunities that exist within the exam-room dialogues between physician and patients.
The in-office conversation between a physician and patient plays a critical role in establishing good clinical relationships, relationships that serve as the building blocks for improved medication adherence and patient satisfaction. However, more often than not, we hear about the dramatic inefficiencies of the doctor-patient encounter. For example, studies have shown that patients can forget up to 80 percent of their discussion with health care providers, and of what patients do remember, approximately half is recalled incorrectly (Kessels [2003] Journal of the Royal Society of Medicine 96:219-222). Fortunately, a relatively new technology-delivered ethnographic research methodology gives researchers a fly-on-the-wall perspective to the natural conversations that occur between physician and patients. This linguistics-based ethnographic approach reveals the conversational gaps that exist within the exam-room dialogue and begins to unravel their roots, allowing the health care industry to bring forward solutions that support and improve the physician-patient conversation and ultimately improve patient outcomes.
Why can unmanned recording of exam-room dialogue be effective?
-
In-office dialogues deliver the point-of-view of both parties in real-time and are not affected by recall bias.
-
Natural language is a true reflection of the attitudes and emotions of the speaker, captured without being affected or influenced by the presence of a third-party observer.
-
Small recorders or smart phones provide an unobtrusive collection methodology, which takes the researcher and their equipment out of the equation. Generally, both physician and patient forget that they are being recorded within 30 seconds of beginning their discussion.
Via technology, a relatively large sample of in-office dialogues can be amassed quickly, developing a database (or corpus) of interactions for research purposes. This large collection of global exam-room dialogues allows researchers to examine a sample larger than what was previously feasible, leading to more concrete findings from the research.
Causes of disparity
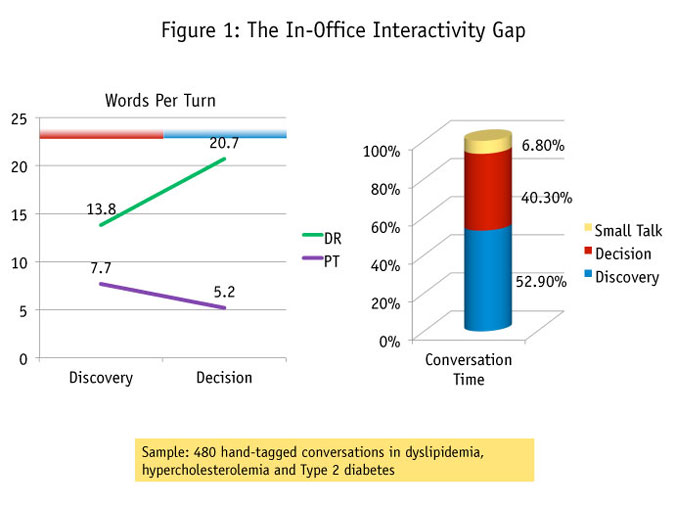
A high-level inspection of exam-room dialogues begins to shed some light on the possible causes of disparity within the exam room. Predictably, physicians tend to dominate the conversation, leaving patients with fewer words per “turn” as the discussion moves from discovery, the phase for exchange of information relating specifically to symptoms and disease experience, to decision, the phase of conversation focused on treatment selection (Figure 1).

But wordy doctors are not the only issue at hand here. All patients walk into the doctor’s office with pre-existing and widely varying knowledge, attitudes, fears and beliefs about their condition which affect a their ability to comprehend new information provided by their health care provider, as well as their willingness to adhere to new treatment instructions. So to truly understand and improve the physician-patient conversation, researchers must go deeper, looking beyond just what was said and how often it was said and examine the linguistic characteristics of the conversation to determine how and why it was said. Through the analysis of large samples of exam-room conversations, trained medical linguists are able to mine the complex spoken language for these underlying patient emotions, identifying conversational gaps and revealing the drivers and barriers of effective communication.
Four conversational gaps
Upon examining thousands of in-office interactions across hundreds of different disease states, four primary conversational gaps between physicians and patients surface:
Gap No. 1: Misaligned treatment conceptualization
Gap No. 2: Dissimilar conversational goals
Gap No. 3: Language disparity
Gap No. 4: Unbalanced decision-making
Misaligned treatment conceptualization
From their candid conversations it becomes apparent that physicians’ conceptualization of disease and treatment differs widely from the way patients view their condition. This gap leads to a misalignment of physician and patient treatment goals, impacting patient acceptance and buy-in to taking medications and modifying their lifestyle.
Physicians generally have a management philosophy in treatment of disease, while patients have a curative approach to treatment. In addition, patients talk about their disease and symptomatology in terms of daily impact (past or present), while physicians focus on a clinical assessment with a future-looking orientation.
In the following dialogue example from a real Type 2 diabetes office conversation, the difference in disease treatment expectations are evident:
Doctor: So, there’s no cure for diabetes; nobody’s getting Nobel Prize pretty soon.
Patient: So, I’ll have it the rest of my life?
Doctor: Correct. You will have it for the rest of your life, yes. Now, unless, again, unless somebody gets Nobel Prize for cure, but it doesn’t look in the near future, so, okay?
Dissimilar conversational goals
Physicians and patients enter the exam-rooms with different agendas for their in-office conversations, affecting the way each participant approaches the conversation and their goals for the visit. Physicians enter the conversation with goals of efficiency, gathering and provisioning only relevant information. Patients, on the other hand, approach the conversation with goals more focused on relationship-building and total information provision.
Societal expectations also play a heavy role in defining the rules of engagement during the exam-room conversation. Physicians operate under the rules of efficiency, objectivity and authority, while patients obey the rules of cooperation, subjectivity and respect. These differences lead to numerous missteps along the way, as physicians try to efficiently collect information and patients attempt to make a relational connection while telling their story (e.g., quantitative vs. qualitative approaches).
Doctor: Tell me about your headaches.
Patient: Uh, lately I’ve had it, you know, a couple of my, you know, migraines, you know, and there’s really no rhyme or reason to them they just, you know, I feel…
Doctor: Are you having more since last time I saw you, you think? You’ve been having more of them?
Patient: Uh, there was like two weeks ago where I went through like three of my Zomig in one week and that’s kind of unusual and, you know, normally, you know, I don’t go through that many in a week.
In this example, the physician cuts instantly to the most relevant information, while the patient tries to provide a more comprehensive overview of his condition.
Language disparity
Physicians commonly speak to patients in “medicalese” – highly technical, clinical language which can confuse and overwhelm patients. They tend to introduce a slew of unfamiliar terms without providing definitions to the patient. Dialogue research shows that this is especially common in specialist conversations such as cancer.
Technical talk is driven by any of several situations, including: physicians are ruled by goals of efficiency due to their busy schedules; physicians are trained as specialists, not educators, and speak in the language they know best; physicians may wish to remove stigma, embarrassment and emotion from the clinical situation, including blunting unfavorable news (e.g., cancer diagnosis communicated through histology).
Here is a dialogue example that shows how the physician’s use of heavy medicalese has led the patient to miss important information regarding recent test results:
Doctor: We did the MRI of the cervical spine and the MRI of the brain. And they compare it the previous ones, which were done in 2008.
Patient: Okay.
Doctor: And based on the findings, so the MRI of the brain was done with contrast and it did show the presence of plaque within the right front and bilateral front of parietal white matter consistent with a known history of multiple sclerosis with acute demyelinative block, there’s an acute block.
Patient: Okay, okay.
Doctor: In the left parietal ventricular white matter. No, so sorry, there was also new lesion in the right frontal subcortical white matter since the prior study.
Patient: Okay. So there’s one on the left and one on the right, is that what I’m getting?
Doctor: Um-hum.
Patient: Because you spoke, uh, you spoke doctorese.
Doctor: Yeah.
Patient: So I don’t always understand, but I heard acute -
Doctor: Yeah.
Patient: On the left and then new on the right.
Doctor: That’s right.
Patient: Okay.
Doctor: That’s right.
Patient: So how do we interpret all of that?
Doctor: That there’s a little bit of progression with disease.
Patient: Okay.
Unbalanced decision-making
Patient involvement in the treatment decision is often minimal. Important aspects such as cost and patient health assessments may be omitted from the office visit, resulting in decisions being made without a patient’s perspective or input.
As shown in the earlier graphic on interactivity (Figure 1), we know that physicians tend to dominate the in-office discussion, particularly as the conversation moves into the discussion of treatment. But what we’ve uncovered through the examination of dialogue is that patients have some conversational shortcomings which allow the physician to steadily take over the conversation at this crucial point.
-
Patients are unsure of their role in decision-making and are uncertain of how to show ownership of their condition.
-
While patients are financially responsible for treatment, cost discussions are largely initiated and guided by physicians.
-
Patients’ knowledge and understanding of treatment options is often limited across therapeutic categories, leaving the physician to make the decision.
The following dialogue example shows the patient’s relinquishing of decision-making power to the doctor, a common occurrence which acts as a barrier to patient-centered decision-making:
Doctor: I’m thinking about adding a second medication in addition to the two tabs of Flomax that you’re taking now. What do you think?
Patient: Well, you’re the doctor.
Doctor: Okay, I’d like to recommend that.
Improve the outcomes
By understanding the top conversational gaps that occur within exam-room conversations, researchers are able to develop solutions that effectively address the gaps and improve the overall experience and outcomes of office visits. One approach is to incorporate the natural language of physicians and patients and respectfully bring together the agendas and roles of both physicians and patients. This also addresses the underlying attitudes and beliefs of both participants and can help guide them to decisions that are mutually satisfying.
The landscape and role of market research is constantly evolving, challenging the entire industry to provide new and innovative thinking to support key business objectives. Now more than ever, research teams are tasked to deliver unique customer insights faster and with less resources. New ethnographic methods such as in-office dialogue research offer the unscripted voice of customers and the ability to reach patient types and geographies not able or likely to participate in facility research. This insight into real, unaided dialogue between physicians and patients can help identify the tipping points that drive exam-room behavior, allowing for even more effective support of the goals of the health care industry.