Improving the long-term prognosis
Editor's note: Based in New York, Thomas Hartley is vice president of research company GfK’s brand and customer experience team.
Over the past several years, pharmaceutical companies have begun leveraging customer loyalty and engagement research to strengthen competitive positionings, improve customer experiences and deliver more engaging marketing. And loyalty research firms have responded with customized innovations geared toward pharma marketers, such as closer integration of brand and marketing concepts into customer loyalty studies.
For pharmaceutical companies, winning the loyalty game means achieving a greater share of physicians who will give your company and product the benefit of the doubt; while creating fewer disloyal physicians – those who will avoid your product whenever possible. Pharma companies have begun to think carefully and act decisively as they move “beyond the pill” and into a multichannel world with a value proposition that integrates the products, resources and services that build engagement and loyalty.
Loyalty research also helps pharma brand teams allocate their wide-ranging marketing expenditures to the most impactful channels and understand which channel attributes are creating levels of dissatisfaction that may ultimately give customers a reason not to buy. Managing physician loyalty does not mean pulling back on marketing activities that lead to short-term sales; it means undertaking additional activities geared to long-term loyalty.
Nearly synonymous
The pharmaceutical industry is different from consumer service and many B2B industries because the medication, not the company, has historically been nearly synonymous with the brand. In banking, retail, technology and medical equipment, the brand of the company has always played a pivotal role – where you shop or who holds your mortgage is crucial. But most pharmaceuticals have been marketed to a fairly small population of specialists, with many companies selling a single brand to any given specialty. As a result, marketing materials and sales representatives have often used only the product’s brand name, so that is all that physicians came to recognize.
Three recent environmental shifts have changed everything:
-
Pharma companies began to market additional products to a given target, first in primary care, then in specialties. A company’s sales representative might speak to a physician about blood lipids one day and acid reflux or pain management the next.
-
Consolidation in the industry presented opportunities to centralize services, from patient education to medical information, and these were branded with the company’s name, not the name of a single product.
-
Competitors began to market very similar products and differentiation came to incorporate not just product features but also the extensive range of services that pharma companies now provide beyond the pill.
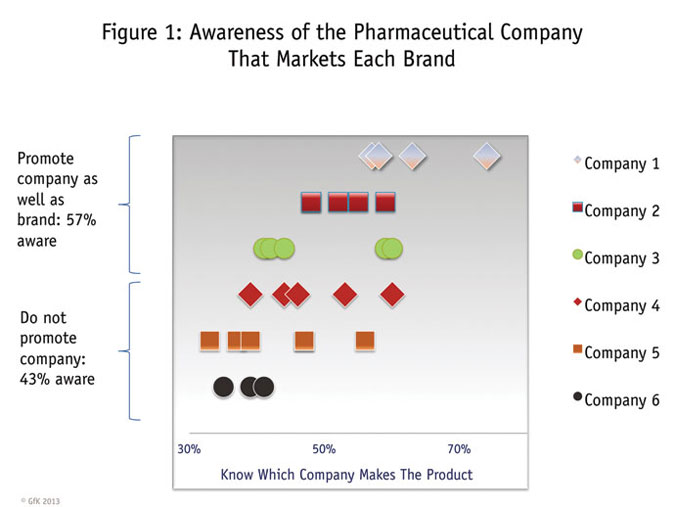
Despite these shifts, some pharma marketers and executives believe that the average physician has no idea which company makes what drug. As Figure 1 shows, there is a wide range of manufacturer recognition. (Each row represents the products made by one company.) The firms at the top have successfully promoted their overall brands and most physicians know which companies make their products. The bottom row shows, however, that there are still medications whose manufacturers are known by fewer physicians.

This complex situation calls for added subtlety in the ways we conduct loyalty research among physicians. Understanding how individual specialties feel about given manufacturers and drugs, and how those relationships are tied to doctors’ interactions with patients, demands greater discernment and higher precision.
Three key elements of this extra dose of insight are:
-
understanding that drivers of loyalty and disloyalty are often different, and measuring them in separate steps;
-
using an index approach to determining physician loyalty, rather than relying on any one score; and
-
recognizing and assessing the multichannel nature of today’s marketing, from video details to social media.
Two-pronged effort
As Figure 2 shows, building deeper relationships with physicians requires a two-pronged effort: converting ambivalent physicians to loyal ones and fixing the problems that are making some physicians disloyal. From a market research perspective, it is important – and somewhat rare – to conduct this analysis in two steps, because doing so requires special non-linear estimators. This analysis reveals an important discovery: The two lists of priorities are not the same. The implication is that different strategies are required to build loyalty and to eliminate disloyalty.

A recent GfK study of pharmaceutical brands looked at which drug brand pillars lead to physician loyalty, with a special focus on strategy: What should the brand stand for in the minds of customers? This study exemplifies a series of studies that were designed to help pharma companies align strategies to build customer engagement. The extensive data set is based on 30-minute online surveys and includes over 4,500 ratings of companies and brands from physicians in over 10 specialties who treat over 15 conditions.
Companies can choose to stand for things that create loyalty – and predispose customers towards their products – or they can stand for things that really have no commercial impact at all. By doing the former, they are occupying the high ground and leaving their competitors to either fight for me-too status or stand for values that have secondary impact.
Differ dramatically
We have worked in a variety of therapeutic areas where the drivers of loyalty, and the most effective channels, differ dramatically. Our recent study looked at the statistical impact of over 20 brand pillars, and should be taken as an illustration; results for each company and brand will differ.
Figures 3 and 4 show the results of the two-step strategic analysis. Two steps are required because our statistical estimator does not assume that just because more of something leads to loyalty it must also be the case that less of that same thing causes disloyalty. Our approach takes more time to explain but the result is that brand teams and enterprises can focus on factors that build loyalty even if their absence is not a negative. And they can determine the dissatisfiers that lead most strongly to disloyalty even if those same factors have diminishing returns.
Figure 3 shows the strongest four attributes in terms of their impact on loyalty – with typical results from this kind of analysis. We learn that physicians are more likely to be loyal if they believe that the company: treats physicians fairly in their interactions; provides a consistently high level of service; delivers valuable services and; understands the physician’s practice.

The bar charts represent the percent of physicians who are delighted with each of three companies. Imagine for a minute that you are Company A. You are faced with Company B, which has convinced over half of physicians that it has achieved excellence in three of the four areas. Your company is fairly close in two of those areas. To create a brand position – a structure of brand pillars that can generate a leadership position in the minds of your customers – you need to find at least one area that you can own. In this case, it will be “providing valuable services.” To complete the bundle, close the gap on those areas where it is feasible, given the size of the gap and the resources that would be required.
Strong impact
Figure 4 shows the four strongest drivers of disloyalty. While one of the factors (understanding the physician’s practice) operates in both directions – and so would have risen to the top in a linear analysis – the other three have a strong impact on disloyalty without having much of an impact on loyalty.

We learn that the strongest driver of physician disloyalty is the belief that a company does not look out for patients’ interests. Another key factor is the perception that the company, its marketing channels and sales force are not focused on physicians’ needs. And a third cause of disloyalty is simply not seeing value in the company’s services.
Company B still dominates, with lower levels of dissatisfaction than competitors on most items. But here, Company A has an area of strength – few physicians believe that it does a poor job of looking out for patients’ interests. So Company A’s first job is to consciously maintain this advantage. Its other job is to eliminate weaknesses (e.g., learning why some physicians believe it does not focus on physicians’ needs) and then take advantage of disloyalty to competitors by demonstrating that it will fulfill this basic need when competitors do not.
We also observe a fundamental principle in action: Three of the four strategies that would reduce disloyalty have diminishing returns. These are areas where problems should be fixed but where creating excellence would not generate a competitive advantage in terms of loyalty.
Measuring and managing
In today’s pharmaceutical industry, where it is no longer the rep and samples alone that build loyalty, the multichannel experience is what creates perceptions of value, strengthening brand pillars and, in turn, developing loyalty (Figure 5). Pharma companies now face the challenge of measuring and managing the entire multichannel experience. Interestingly, in different therapeutic areas, very different channels have assumed the mantle of supporting actors that supplement the leading role of the rep. This article presents one example.

Drill-down analysis identifies channels that have the strongest impact on perceptions of your company – those channels that lead physicians to see your firm as delivering any or all of the key loyalty (and disloyalty) drivers.
Figure 6 shows a channel drill-down analysis for one critical brand pillar: “provides valuable services.” It will not surprise anyone in pharma that the sales rep is the strongest pillar. Samples also are critical, in those therapeutic areas where samples are a way that physicians can provide valuable support to patients. But many other factors now play a role, from video details to medical liaisons to patient assistance and the entire spectrum of resources that has created the multichannel customer experience. This shows how a multifaceted and intricate brand-building process can be simplified by prioritizing high-impact channels that strengthen a brand pillar and lead to loyalty.

To build the perception that the company provides exceptionally valuable services, marketers need to pay attention to the top-box ratings of each channel that leads to the perception of excellence in those brand pillars that support loyalty. Our results show that Company A will need to focus its attention on video details (similar to a sales rep visit but conducted on an audio-visual platform) and sampling. This company’s reps and Web site are providing an outstanding experience for many physicians. But the percent of physicians giving the highest ratings on video details and samples is sub-par.
Customer loyalty and multichannel customer experience research tells you what areas need to improve, in the context of the full marketing program, to ensure that investments have the biggest impact on building loyalty and share of scripts. Additional qualitative research, competitive analysis or strategic innovation will help the brand teams determine specifically how to improve. Only by taking a holistic look at all of a company’s physician touchpoints, in combination with a loyalty assessment that shortens that list of touchpoints into a focused and manageable set, can we arrive at a true understanding of how to allocate efforts and investments.
Metrics vary widely
As in other industries, the metrics used to measure loyalty in health care vary widely. Net Promoter is the most famous metric, fleshed out in Fred Reichheld’s publications and Bain’s consulting work, while satisfaction is still the most common. But any loyalty metric needs to be carefully considered.
The critical question is how much benefit accrues from the additional complexity of an index, compared to the simplicity of a single question. The pharmaceutical industry is rich with data on actual customer behavior, including scripts written or revenue resulting from an individual physician’s prescribing behavior. Figure 7 shows the results of an analysis in which physician opinion data is merged with actual prescription revenue per physician. Each pair of bars compares loyal physicians – however measured – with physicians who are not loyal.

In each instance, the loyal physicians (represented by the orange bars) are responsible for more revenue per physician than the ones who are not loyal (the gray bars). The key question is: How much more revenue? Comparing Promoters to Detractors achieves a 25 percent differential, which is to say that Promoters prescribe 25 percent more than Detractors. (Promoters selected 9 or 10 on the recommendation scale, whereas Detractors selected 0 to 6.) When we apply the same scale and calculation to a satisfaction question, it discriminates somewhat better, with extremely satisfied physicians (scores of 9 or 10) prescribing 35 percent more than not-very-satisfied ones (those who chose 0 to 6).
Opinion researchers have known for years that indexes outperform individual questions, so it is not surprising that the loyalty index outperforms the single-question items. But by how much? Loyal physicians (defined as scoring above a threshold on the index) prescribe 55 percent more than physicians who are not loyal.
It is important to note that all three of the indexes generated roughly the same percentage of physicians who were considered loyal. They differ on which physicians were placed into the loyal category. In pharmaceuticals, at least, an index is a more accurate measure of loyalty, if what you are interested in is more prescriptions and more revenue.
And a more accurate loyalty metric will lead to more precise driver analyses. Driver analysis determines for which variables a high score on the attribute coincides with a high score on the loyalty metric. If your loyalty metric is not accurately predicting future prescribing behavior, the drivers will be off, too.
Leads to more prescriptions
In undertaking and deploying customer loyalty and engagement programs, pharmaceutical brand teams and multichannel marketing executives have added a longer-term and customer-centric focus to their existing promotional and service activities. They have discovered that intentionally building brand pillars – the things that your company and your brand stand for – is vital. Putting in words the things that you stand for, and making sure that physicians experience and recognize those benefits, leads to more prescriptions than a focus on short-term promotional activity alone.
In accomplishing this, pharma companies have also viewed their mix of promotional and service activities through slightly different lenses. The ability of a channel to drive and maintain scripts and share will always remain primary. However, we have now learned that it is also important to ensure that the mix of channels supports your brand pillars and creates loyalty. And ensuring that customers are satisfied with their experiences with those channels will lead physicians to prescribe more of your brand because of – and not despite – the things that you stand for.