Editor's note: Eelke Roos is a senior research manager at SKIM London.
Have you ever wondered why people choose Coke over Pepsi or Bud Light over Coors Light? Or why two brands of pharmaceuticals with similar efficacy and safety measures are prescribed differently? The reasoning behind these types of decision outcomes is often more influenced by emotion than rational thinking.
While both are effective ways of processing information, feeling is more immediate. The interplay between rational and emotional decision-making reveals what actually happens at the tipping point – in this case, the point at which a prescription is written. One would expect physicians to rely primarily on hard facts and objective data but that is often not the case. In exploring how these decisions are really made, it is necessary to identify when and how rational and emotional processes come into play. And, compared to more traditional market research tools such as in-depth interviews in a research facility, mobile devices are superior research tools for revealing the true in-the-moment drivers behind prescribing decisions.
To understand why these developments in mobile research are of interest to health care market researchers, it is helpful to understand groundbreaking decision-making theories of the last few decades. In that time, we have gained a much richer understanding of decision-making thanks to pioneers like Nobel Laureate Daniel Kahneman. In 2002, Kahneman was the first psychologist to win the Nobel Memorial Prize in Economic Sciences. In 2011, he published his book Thinking, Fast and Slow, which advanced our understanding of decision-making. Kahneman explains why people sometimes make seemingly odd and irrational decisions and what may elicit these types of decisions.
The main driver behind Kahneman’s theory of decision-making is his observation that decisions can be heavily influenced by emotions and don’t always follow the rules of rational thinking. Kahneman is regarded as a pioneer in this new age of understanding decision behavior and is recognized as the father of behavioral economics. His theories are important to market researchers as they offer an appealing explanation for why customer choices cannot always be predicted using rationalized models and why certain brands do better than others even though they don’t necessarily provide better products.
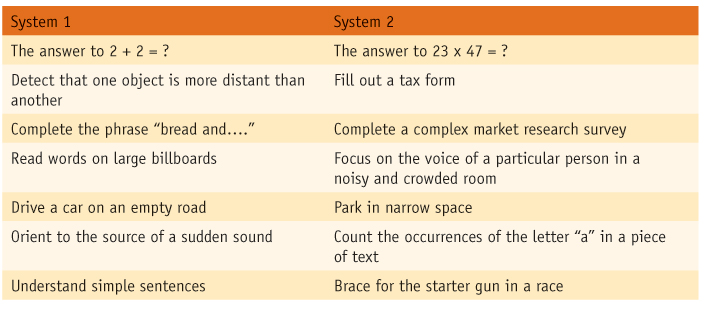
Kahneman divides thought processes into what he calls System 1 and System 2, or the “dual-process” model of the brain. System 1 is fast, intuitive and emotional, can’t be switched off and is the “secret author of many of the choices and judgments we make. System 2 is slower, more deliberative and more logical.
In order to better understand these two different modes of thinking, consider the following small exercise involving two different calculations.
Here is the first calculation: 2 + 2 = ?
It is not difficult to automatically arrive at the answer: 4. The answer comes easily and requires minimal cognitive strain. This is System 1 at work. Another term for System 1 is “intuition.”
Now, let’s perform another calculation. Please take a minute to do it (pencil and paper are allowed): 23 x 47 = ?
This time it was not as easy to come up with the answer. When doing the calculation, you most likely experienced cognitive strain and an answer did not come to mind immediately. If we monitored your biological functions, we would have seen that your heart rate and blood pressure went up, your pupils became dilated and your sweat glands were activated. This is your System 2 at work.

When asked if 198,459 is a possible answer, your System 1 thinking (intuition) would intuitively tell you no. It would also tell you that the answer is most likely not 156. However, System 1 does not have an exact answer to this problem readily available. It would also not know if 1,231 is the correct answer, were it given as an option. In order to get to the answer, you needed to switch on your System 2 thinking and exert some effort to figure out that the answer is 1,081. (One can explore this theory further by visiting www.theinvisiblegorilla.com/videos.html. Follow the instructions faithfully to discover how System 2 takes over, rather unwillingly, when things get difficult.)
The table shows a list of various types of decisions that are characteristic to both System 1 and System 2.
System 2 is thought to be quite lazy and only comes into play when we need to make a difficult decision. System 1, by contrast, is automatic and unconscious and hums along continuously in the background. It constantly surveys the environment and processes the incoming stimuli with high speed.
Because System 2 is lazy, you instinctively try to make decisions with System 1.
Interestingly, through practice, humans can convert System 2 activities to become System 1 activities. While a game of chess requires great concentration for a chess player with average skills, seasoned chess masters make their potential moves almost automatically and do not experience the same cognitive strain. For chess masters like Garry Kasparov, a standard game of chess is more a System 1 activity than a System 2 activity.
Prescribing drugs becomes an automated activity
So, which thinking mode influences physicians’ decisions? During medical training, seeing patients and prescribing treatments is a strenuous activity that requires a great deal of concentration. However, more tenured physicians make a majority of their prescribing decisions seemingly effortlessly. Over time, prescribing drugs becomes an automated activity that is more driven by System 1 than System 2 thinking. System 2 is only activated in rare cases. In clear-cut patient cases, a physician immediately and instinctively knows which drug to administer. With little cognitive effort, they are able to make a prescribing decision, similar to a chess master who relies on System 1 thinking to make his next move.
System 1 decisions are heavily influenced by emotions and often diverge from rational thinking. Kahneman describes many experiments in his book that prove that System 1 is not rational but emotional. If one can conclude that prescribing decisions are typically a System 1 activity, that means these decisions are heavily influenced by emotions. Therefore, if one tries to obtain a deep understanding of the reasons behind a prescribing decision, System 1/System 2 theory tells us that researchers need to capture the emotional as well the rational part of the decision making process.
One challenge of measuring emotion (System 1 thinking) is that the emotion itself, and the recollection of the emotion, tends to dissipate quickly. Emotion has to be captured and measured quickly in order to maximize research results. Because of the time lag involved, research projects involving physicians are designed only to uncover the rational (System 2) aspects of a decision and not the emotional aspects (System 1). For example, we often ask physicians to take patient forms to a research facility and explain why they made a particular treatment decision.
To get to the truth behind a prescribing decision and to understand the emotions that are often driving such a decision, it is important to conduct the measurement as close to the actual occurrence as possible. Without an understanding of the System 1 aspect, we only get a partial understanding of the drivers behind the decision. While measuring close to a point of action is more easily done with consumers (e.g., by following a person on a shopping trip), with physicians it is extremely challenging.
Emotions are still fresh
Since observing a physician while he or she makes a prescribing decision is usually not an option, mobile solutions are the next best thing to being there. While online surveys are traditionally completed using a desktop computer, a mobile device enables the respondent to complete a simple survey immediately after seeing the patient, when emotions (System 1) are still fresh.
In a recent case study, SKIM researchers conducted research for a brand team at a well-known pharmaceutical company with the following objectives: track the prescribing of oncology treatments over time along with patient characteristics driving the prescribing decision; understand why certain brands were being prescribed and not others.
There was a general feeling among the brand team that conventional research methods were too general and did not reveal the full story behind why certain brands were being preferred over others, therefore they were open to trying a novel methodology. For example, when physicians were invited to a research facility and asked to describe their reasoning regarding a particular prescribing decision, the responses were usually very clinical and devoid of insights regarding any non-clinical or lifestyle-related feedback. Because the study featured agents that were very similar in efficacy and safety (virtually interchangeable, in fact), researchers felt there must be an extra layer of reasoning regarding the prescribing decision.
SKIM researchers deployed a mobile survey app that could be easily and quickly accessed by a physician directly following a patient consultation. The survey app was designed to take no longer than five minutes. By keeping the survey short, physicians could answer survey questions between consecutive patient consultations.
The survey app consisted of two main parts: 1) a voice memo during which respondents were asked to record their reasons behind the decision; and 2) short, closed questions (single-select, multiple-select and rank) to gather relevant patient data.
For the audio recording, the respondents were asked to share the following information: clinical history of the patient; summary of what was discussed during consultation; treatments considered by the respondent during consultation; treatment chosen and reasons why; and reasons for not choosing any of the other treatments.
During recruitment, respondents were thoroughly briefed on how to use the app and how to record the voice memo. They were advised to provide a certain depth of information as well as an approximate length of time to spend on each aspect of the voice memo. Because the research had a quantitative component, the required sample was relatively high, making a thorough briefing ever more important to ensure adequate participation.
Came prepared to challenge
At the conclusion of the study, researchers collected and analyzed more than 500 patient cases, including voice memos, from physicians in the U.S. and Europe. Since the patients were diagnosed with an oncologic disorder, the consensus was that treatment decisions were related to clinical outcomes and patient characteristics. The mobile research revealed the extent to which patients were involved in treatment decisions. In many cases, a patient declined a treatment or came prepared to challenge the oncologist on his or her choice. While the team was aware that this sometimes happened, the high frequency of occurrences was a novel insight that warranted further research into what patients want and how to convey this information through DTC (U.S.) or sales reps.
Unlike in-depth interviews, follow-up questioning is not possible with in-the-moment mobile research. While this presents some limitations, in this case it led to a very actionable insight that directly influenced the brand’s marketing strategy. We learned that the drug produced by the client company was not top-of-mind when discussing options with patients. Physicians very often presented multiple options to the patients (the frequency of this was an insight on its own) and discussed with the patient which drug to prescribe. Among the options often excluded was the client’s drug. It was clear that the brand team needed to increase awareness of the drug.
Because researchers collected quantitative data on patient characteristics, they were able to create crosstabulations showing which drugs were prescribed to which patient types. The client drug in question was indicated for patients with very specific disease characteristics. The research revealed that the client drug was often not presented as a treatment option even though many of these patients were presented with multiple options and were engaged in the decision-making process. In addition to the much-needed increase in overall awareness, it was clear that an educational campaign was required to educate and remind physicians which patients are most suitable for treatment with the drug.