Editor' note: Zoe Dowling is lead research strategist in the Los Angeles office of Stamford, Conn., research firm FocusVision. Ana Tereza Horta is projects director at Albar Research, Sao Paulo, Brazil.
 Latin American countries have historically had a troubled relationship with nutrition and food supply. For many years, hunger, malnutrition and its consequences impacted mortality and the quality of life negatively across the region. However, in recent years, we have seen a radical shift. On the one hand there has been a significant decrease in incidences of those diseases that are characteristic of poverty and food shortage. On the other hand, there has been an increase in obesity, not only among adults but also – and most concerning – among children.
Latin American countries have historically had a troubled relationship with nutrition and food supply. For many years, hunger, malnutrition and its consequences impacted mortality and the quality of life negatively across the region. However, in recent years, we have seen a radical shift. On the one hand there has been a significant decrease in incidences of those diseases that are characteristic of poverty and food shortage. On the other hand, there has been an increase in obesity, not only among adults but also – and most concerning – among children.
Good eating habits in childhood build good eating habits throughout those children’s lives. That is why childhood obesity is so disturbing. An obese child has 60 percent chance of becoming an obese adult, which may lead to several life-threatening diseases and a low quality of life.
A study by the World Health Organization (WHO) showed that as a whole, Latin America has the largest proportion of overweight preschoolers, compared to African and Asian developing countries. Specific numbers include the 120 percent growth of child obesity in Brazil over the last 20 years. The estimate is that 30 percent of children in Brazil are now overweight or obese. Mexico is already considered the No. 1 country in the world for child obesity.
Three questions
In 2016, Stamford, Conn.-based research company FocusVision joined forces with Brazil-based Albar Research to conduct a study to understand the trend towards childhood obesity in Latin America and what could be done about it. The team sought a comprehensive and in-depth understanding of the region’s child obesity problem. There were three core questions they wanted to answer: What is the distance between a child’s real and their “ideal” diet? What prevents children from having the ideal diet? What needs to be done to fight obesity?
In order to get to the answers, the team investigated current diets, the key factors for their diet choices and what would be the ideal diet from the family’s point of view.
Covering Brazil, Mexico and Colombia, they targeted sample with a geographical spread so as to be representative of the general population in those countries.
The team not only wanted to investigate thoughts, opinions and emotions of parents but also to see firsthand their children’s daily habits and routines. They also wanted to hear from the experts: health care professionals closely involved with managing and treating children’s weight and nutrition. Getting this full view required an integrated approach, mixing both qualitative and quantitative techniques over three phases.
Phase 1 – IDIs: Getting the experts’ perspective
The project started with one-on-one, in-depth interviews (IDIs) with pediatricians, endocrinologists and key opinion leaders. These lasted approximately one hour and covered topics that included parents’ and children’s nutrition behavior, motivation and factors impacting diet as well as obesity problems and treatments. The interviewing technology allowed the team to engage respondents remotely all over the countries involved, face-to-face via Webcam, and enabled the moderator to present stimuli to enrich the discussion.
Phase 2 – Listening to the parents
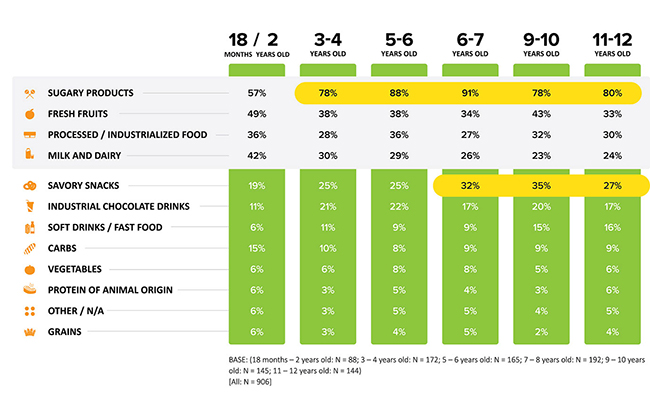
For this stage, the team carried out a 30-minute online quantitative survey with parents of children between 18 months and 12 years old using FocusVision’s Decipher platform. Neither the children nor anyone in the household could have a health problem, except for a family history of obesity, but they did not need to have the risk of obesity to participate. We asked respondents about their child’s current eating habits (food choices, daily routines, eating times, etc.) sources of nutrition knowledge and support, grocery shopping attitudes and behaviors and ideal diet. The quantitative data helped us to understand the prevalence of different food groups in children’s diets (Figure 1).
Phase 3 – Exploring and engaging with families inside the home
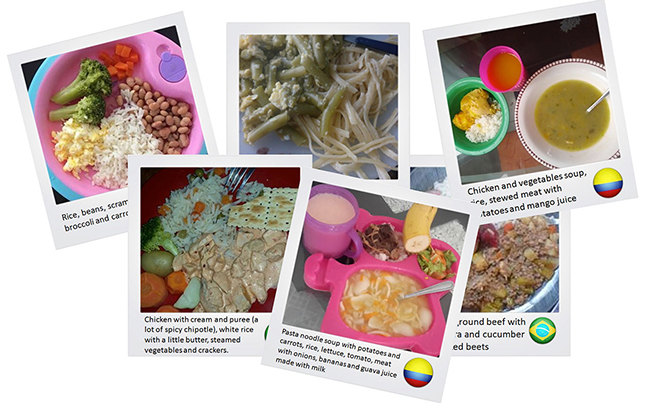
Sixty participants from the online survey were selected to take part in this third phase. Using a digital mobile and Web platform allowed consumers to engage in qualitative research activities, such as mobile diaries, insight communities and bulletin boards, with the ease and style of their favorite social media app. Through journals, with images from their meals (Figure 2) and other interactive activities, they were able to have a full and detailed conversation about daily eating habits.
Chubbiness is a sign of health
In Latin America in general, there is a perception that a chubby kid is cute and that a bit of chubbiness is a sign of health. According to the WHO, 70 percent of obese children’s mothers only consider their child “chubby.”
But not knowing that their child has a health problem that needs treatment is only the tip of the misinformation iceberg. Parents are still lacking enough information about proper nutrition. It starts with their own eating habits, which are usually very bad. Children tend to replicate their parents’ tastes and behaviors. Instead of setting an example, parents want kids to eat what they don’t eat themselves. Many physicians told stories about how parents are not willing to change their lifestyles. This was the main challenge for parents and physicians: changing habits and breaking behavior patterns that have been carried out by generations. According to the professionals, the best way to convince families to break behavior patterns is by making them truly understand the importance of this change and the consequences obesity can bring: diabetes, high blood pressure, pulmonary and cardiovascular problems, just to name a few. When parents get scared, their behavior can change.
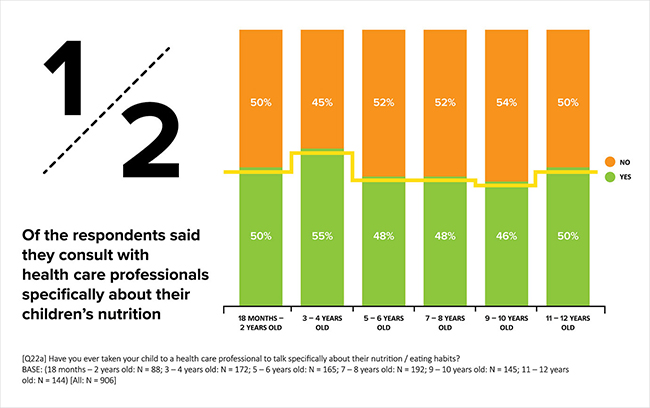
The research also found that parents don’t always refer to a professional for guidance and hence end up mistaken as to what is appropriate and healthy food for children (Figure 3). Public health care systems are overwhelmed and unable to meet the demands of large populations, making access to guidance a problem. The misinformation is not only about what obesity is and the kinds of problems it may bring but also about what healthy food actually is. We learned from experts that many families consume processed powder juices and “baked snacks” (such as potato chips, for example), believing they are making healthy choices.
One big indicator of this lack of information is that most parents who participated in our survey said they were confident that their children’s diet is balanced. However, they also admitted to often giving their children soft drinks for lunch and sandwich cookies, chocolate and chocolate drinks for breakfast (lunch and breakfast being, in this order, considered by them the two most balanced meals).
Important gap
It was very interesting to notice that, after responding to the survey, and then completing the meal journal for a week and hence giving the topic much thought, respondents realized that there is an important gap between the ideal diet and real life. At first, they always said they give their kids the best possible nutrition but after putting everything “on paper” they realized they could do better. That is when many of the parents felt that they needed more guidance in order to get things right.
But it is still not that simple. There are other problems to add to the mix. Parents working full-time, without enough time to prepare and have meals with their children, need to entrust this responsibility to a third party, who might not be so concerned about the quality of the food offered. And thus, many times frozen meals are the solution. In addition, full-time working parents often feel very guilty about not spending enough time with their kids and so give them everything they want and don’t establish firm boundaries (in Latin American cultures, food is deeply related to leisure and family time).
Plus there is an increase in sedentary lifestyles. Children stay indoors more and like to play video games. Tablets and smartphones are widely used by busy parents to distract children who sometimes just need to move a little bit more.
As if all that was not enough, many health practitioners mentioned that kids up to the age of 10 do not have any vanity about their bodies, so being chubby is not something that seems like a problem for them. Moreover, they are constantly exposed to media that shows them ads for sugary, processed fast food.
This is the complex equation leading to obesity in all layers of Latin American society – from the highest to the lowest socioeconomic levels. Lower classes have difficulty accessing healthier foods since they are usually more expensive than the ultra-processed food with lower nutritional value. And the higher socioeconomic families have a very active social life (birthday parties, movies with popcorn and soft drinks, restaurants, etc.,) and so tend to indulge more.
Potential economic problem
The overwhelming increase in child obesity in Latin American countries is disturbing as a public health issue itself but in economic terms it is also a potential problem. According to the Organization for Economic Co-operation and Development (OECD), an obese person incurs 25 percent higher health expenditure than a person of normal weight in any given year. Obese people earn up to 18 percent less than non-obese people.
The best way to overcome obesity, our respondents agreed, is through education and awareness, not only at home but also in schools.
It’s clear that several stakeholders have a shared responsibility in this challenge. Governments need to build awareness campaigns, encouraging a better structure and access to the public health care system and creating tax programs to encourage local, organic food production and hinder access to industrialized, ultra-processed food. Schools need to be involved with educating children about nutrition, the problems and dangers of obesity and the value of maintaining their health and good eating habits. The media could be encouraged to limit space for advertising unwholesome foods and give more space to nutrition education campaigns. Parents and relatives need to be educated and willing to change habits as well as being more clear and consistent with children when feeding them. Finally, health care professionals must continue to provide guidance and inform people regarding all the implications of good and bad eating habits.
An integrated approach across all these groups should drive a change in behavior and ultimately have a positive long-term impact on health and the economy.