Be there for them
Tom Donnelly is MedTech director at the Research Partnership. He can be reached at tom.donnelly@researchpartnership.com. Dan Buckley is field director at Just Worldwide. He can be reached at dan@just-worldwide.com. Amanda Pirraglia is associate director at the Research Partnership. She can be reached at amanda.pirraglia@researchpartnership.com. Andrew Watson is director, business insights at PTC Therapeutics. He can be reached at awatson@ptcbio.com.
As technology advances there is a growing array of MedTech solutions – wearables, voice-activated devices, telehealth, etc. – to better support patients in their daily lives. However, MedTech research with rare-disease patients presents several unique challenges that must be considered. Ideally, interviews would be in-person in a central location to observe device use; the rarity of the condition can lead to the need for a hybrid methodological approach. In this article, we will: provide some background on rare disease and how research can be different in this population; describe different methodological approaches, respondent configurations and recruitment considerations; and discuss aspects of moderation and analysis.
Background
A rare disease affects less than 500 in 1,000,000 people (0.05% prevalence). Definitions vary slightly: in Europe, a rare disease affects less than 1 in 2,000, while in the U.S. it affects less than 200,000 people.1 Overall rare diseases affect up to 6% of the world population (~1 in 20) and about 80% of rare diseases have a genetic origin. Sadly only ~5% have an approved treatment.2
Further subclassification can help to define those indications that are ultra-rare or those that have orphan disease status. The definition of an ultra-rare disease in Europe is that it affects less than 20 in 1,000,000, while the U.S. has no distinction for ultra-rare.3 Approximately 85% of the rare diseases have an incidence of less than 1 in a million (0.0001).
Orphan status may be for a rare or common condition (e.g., malaria, which has 3 million cases/year). Often, they are for rare diseases because of a small patient universe making it harder to conduct clinical trials. In the U.S., the Orphan Drug Act (1983) provides incentives for the development of drugs to treat rare diseases including seven years of market exclusivity after approval.
Unique frustration with rare diseases
How are rare diseases different? There can be a lot of unique frustration with rare diseases, both for patients and health care practitioners (HCPs). Patients may have been searching for some time and been shuffled among different HCPs and complementary care, possibly having been misdiagnosed and/or dismissed along the way. By the time they receive their right diagnosis, some feel vindicated (“I told you so”) and relieved. However, they may feel that the general population does not understand their condition or have empathy for their experience. Even once a proper diagnosis is made, there may be limited options for treatment and often no cure. This can make dealing with the rare disease unfulfilling for HCPs and extremely frustrating for patients and caregivers. Additionally, having a community to turn to for educational and emotional support is essential, but even after a proper diagnosis, patients with rare diseases may find that support is limited, preventing them from connecting with other patients, caregivers or access to health care.
For general practitioners, and even some specialists, symptoms of a rare disease may resemble other more common diseases or may be something they have never seen or even heard of before. For many rare conditions, education throughout schooling on the disease may be limited. We have heard doctors express that a condition in its entirety was covered in one class setting in medical school because of its rarity, thus preventing them from identifying the symptoms in practice when presented with a patient case.
Doctors themselves are also frustrated with the unmet support and treatment needs for their rare disease patients. Two specific areas where our hybrid MedTech approaches have been used to provide insights on these unmet needs are Friedreich’s ataxia (FA) and spinal muscular atrophy (SMA).
Friedreich’s ataxia is a rare, inherited, degenerative disease.4 It damages the spinal cord, peripheral nerves and the cerebellum portion of the brain. This condition tends to develop in children and teens and gradually worsens over time. Unsteady, awkward movements and a loss of sensation due to nerve injury develop as the disease progresses. Symptoms of Friedreich's ataxia often start between ages 5 and 15, although they can develop later in life.5 Symptoms include: trouble walking, possibly the need for a wheelchair; limited dexterity and fine-motor skill; tiredness; slow or slurred speech.
Spinal muscular atrophy is a disorder affecting the motor neurons – nerve cells that control voluntary muscle movement.6 These cells are located in the spinal cord. Because the muscles cannot respond to signals from the nerves, they atrophy – weaken and shrink – from inactivity.
SMA is classified into four different types that appear as a scale of severity, where Type 1 is the most severe and typically presents with symptoms within the first six months of infancy, while Type 4 rarely has an impact on life expectancy.7 One in every 6,000 babies is born with SMA. It is one of the most prevalent genetic disorders affecting young children and a major cause of death in infancy. SMA can strike children in infancy or as they grow into adolescence. SMA in infancy and early childhood is associated with worse outcomes, while patients who develop symptoms later in childhood or in adolescence usually have a more positive prognosis. Symptoms include:8 weakened muscles closest to the center of the body, including the shoulders, hips, thighs and upper back; difficulty breathing and swallowing.
Approaches to rare-disease patient research
Conducting marketing research and human factors with rare-disease patients is challenging for many reasons. First, it is ideal to conduct the research in-person in a central location facility to observe device use. This allows the research team to discuss feedback live, as well as be on-hand to fix any malfunctioning devices. However, due to the rare nature of these conditions, recruiting a reasonable sample size into a given research location is unlikely. Second, the abilities of respondents may be limited depending on the severity of their rare-disease symptoms – which can vary within a given condition. For example, FA patients have increasing dexterity challenges over time, which will impact their ability to manipulate a medical device. As another example, SMA patients with muscles that have started to atrophy may have difficulty sitting up through an entire interview.
Given such challenges, both the methodology and recruitment must be flexible, allowing a combination of in-person interviews in a facility, in-home interviews and virtual interviews. As shown in Figure 1 and described below, there are advantages and disadvantages of each approach. In addition, a combination of interviewing patients and/or caregivers should also be considered. In some conditions, interviews with patients can be difficult, such as pediatric patients or those with cognitive deficits. Having a caregiver participate can aid in gathering feedback. We will review these interview methods and respondent configurations.
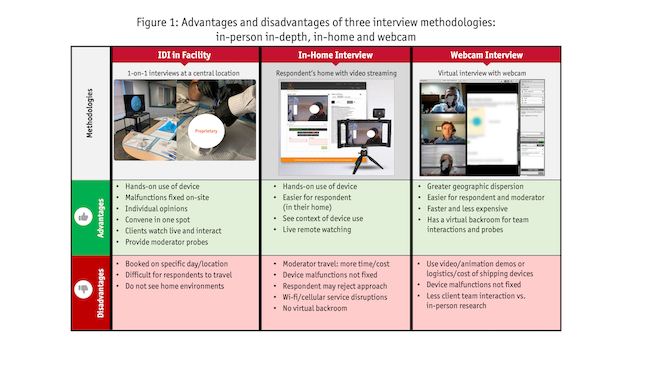 Interview methods. The gold-standard interview method is the in-person in-depth interview (IDI) in a central location facility with clients observing in the backroom. There are many advantages in conducting MedTech research with this approach. Most importantly, this allows hands-on use of devices you are testing. The client team can watch live as a group to discuss insights and provide feedback to the moderator. Clients are less likely to be distracted, as they might be in their work or home office. In addition, if a device breaks, the research team is on-site to make the appropriate modifications.
Interview methods. The gold-standard interview method is the in-person in-depth interview (IDI) in a central location facility with clients observing in the backroom. There are many advantages in conducting MedTech research with this approach. Most importantly, this allows hands-on use of devices you are testing. The client team can watch live as a group to discuss insights and provide feedback to the moderator. Clients are less likely to be distracted, as they might be in their work or home office. In addition, if a device breaks, the research team is on-site to make the appropriate modifications.
Though the most efficient method, there are disadvantages to consider with in-person interviewing. Given that the research is conducted on a specific day in a specific location, respondents, clients and researchers must all travel and be on schedule. Doctor and other types of health care appointments may be frequently on calendar for rare-disease patients, thus causing a disruption in potentially having to rearrange appointments to accommodate both the travel and time needed to participate in the interview. Patients may be reliant on their caregivers to assist them in participation, thus potentially having to consider accommodating caregivers’ schedules as well. Travelling may be particularly challenging for respondents, such as those with mobility or accessibility issues (e.g., FA, SMA). And finally, you lose the opportunity to observe how the patient interacts with the device in their home environment.
Conducting interviews at a patient’s home provides important real-world context of the medical device use, which can have implications for device design. If you include video streaming, clients can engage in the research and provide live feedback during the interview. As with IDIs, you get feedback from respondents with hands-on use of the device. This approach is easier for respondents because they do not need to travel, however, travel for the moderator can be taxing, expensive and lengthens the timeline. While clients can watch live, there is no virtual backroom and there can be disruptions in the signal due to unstable wi-fi/cellular signal. When devices malfunction, client engineers are not on-site to fix them. Also, additional compliance considerations are needed (e.g., consent from others in the home, personal information shown on camera) and respondents may reject the approach because of privacy issues.
Webcam interviews are a popular alternative, where you conduct a virtual interview through a platform using a webcam. With device testing, you need to use virtual stimuli (e.g., images, animation, videos) or ship devices to respondents. This approach has the potential advantages of having a wider geographic dispersion of respondents, as well as being able to field more quickly and be lower in costs due to no travel. The approach is easier for respondents, moderators and clients because there is no travel required. Most virtual platforms have a virtual backroom, allowing client interactions and moderator probes. However, clients may be less engaged compared to attending in person research.
Regardless of the interview technique chosen, it is essential for the moderator to be trained in using the device before fieldwork commences. The moderator should ideally have the opportunity to test the device on their own time to play around and become familiar with its functionality. At the very least, a training session on how to appropriately use the device should be required, so that if patients have questions on it while in field, the moderator can properly address.
Device shipment logistics. Shipping medical devices for research takes planning, added time and costs. You must consider the geographic locations (e.g., U.S., EU5, other) and type of equipment/materials. When shipping internationally, review the specific customs rules for each country. A key logistical issue experienced when shipping devices is airports retaining the devices when the contents contained within the box are unclear or potentially considered hazardous. This can especially be a hassle when transporting the devices internationally. You will need detailed documentation of what is in each box with counts, along with the purpose of the market research. This detail written on a letterhead could help formalize the transport. If you are shipping through mail to respondents (e.g., for webcam interviews), you run the risk that they do not ship it back or that it gets lost in mail. For more information, see a prior Quirk’s article, “Stimulating simulations: strategies for conducting global device testing” (November/December 2021).
Another potential challenge to consider with device logistics is its functionality, particularly if the devices break. In that instance, the interview would need to be rescheduled after a new device is delivered. We have had success using a courier service to speed up field time; however that adds additional cost to the budget. For more information on this approach, see a prior Quirk’s article on virtual observation: “Watch and learn: the power of observation and iteration” (May/June 2021).
Respondent configurations. When conducting research with rare-disease patients, the respondent configuration needs to be flexible, whether you interview only the patient, only the caregiver or both together. Each individual approach has advantages and disadvantages, as shown in Figure 2 and detailed below.
 Interviewing patients provides an in-depth, unbiased, individual opinion in the patient’s own perspective. Interviewing the caregiver will be needed if the patient has a cognitive deficit, is too young to be interviewed or has passed away. They can give their in-depth, unbiased, individual opinions from their perspective. Sometimes the caregiver knows more than the patient. However, the caregiver is not the patient.
Interviewing patients provides an in-depth, unbiased, individual opinion in the patient’s own perspective. Interviewing the caregiver will be needed if the patient has a cognitive deficit, is too young to be interviewed or has passed away. They can give their in-depth, unbiased, individual opinions from their perspective. Sometimes the caregiver knows more than the patient. However, the caregiver is not the patient.
Research can be done with both the patient and the caregiver. In this way, you can get the best of both worlds, receiving both points of view. Also, they each may remind the other about forgotten information (e.g., which specialist they went to initially versus getting a final diagnosis). This approach is useful when interviewing children – because you can get their input with the help of parent – as well as for those with cognitive deficits. Both the patient and caregiver have different milestones that are important and specific to them in their journeys, so interviewing both allows you to capture both and compare and contrast the milestones. The downside of this approach is that respondents can bias each other. A workaround is to have part of the interview with only the patient, part with only the caregiver and part with both. Of course, this leads to a longer interview.
Recruitment considerations. Recruitment for rare-disease patients is particularly challenging due to the rarity of the condition. Beyond the flexibility mentioned in the research method and respondent configurations, the recruitment criteria must also be considered. Longer timelines and larger budgets will also be required compared to more traditional conditions.
The recruitment team should select the most suitable recruitment models depending on project requirements, cultural nuances and legal requirements. Some approaches include clinical, advocacy, media and technical outreach, as well as targeting areas with treatment centers. Using clinical outreach to find the right patient through health care professionals is often an effective approach. While this will add to the costs of the recruitment, it ensures the correct patients are identified. Advocacy outreach is used to find the right patients through non-clinical support networks. This was extremely useful in the past but there is significant variability in the size and engagement of these advocacy groups in the rare disease space. Using online groups is often more effective and is more geographically diverse. This can lead to extra cost and time but can enrich insights. Media outreach through film and animation to deliver promotional material relating to the project both for the finder and patient efficiently expands the reach of recruitment effort. Efforts using technological outreach for precision targeting of knowledge leaders, health care practitioners and sites within given geography is also effective. Another approach is targeting areas with key treatment centers to find enough respondents close to one another and able to refer others in their area.
For every project, there are also situational considerations that may impact what approach may be best. For an at-home project in 2022, recruitment and research methods had to consider patients’ concerns with COVID-19. Significant time was spent with each patient to reassure them of the moderator's vaccine status and taking tests to be sure they felt comfortable. The issue may not always be a pandemic but each project has its own unique considerations for the time needed for individual challenges to be addressed. The research and recruitment teams need to be patient-centric with individual understanding and flexibility. The team should account for ample time to ship devices and/or for moderators traveling for in-home research.
Approaches to moderating
As with all qualitative research, moderating skills are key to success. For patient research, it is especially important to keep certain factors in mind and find ways to overcome those challenges. Given it is a rare disease, the patient may have never participated in marketing research. In this case, it is vital to first build rapport with each patient. As a simple example, when you ask about their hobbies or other background information, be sure to relate to a detail with something about yourself, such as a related hobby.
As discussed with recruitment, all parties (recruiter, moderator) must be privy to what each patient desired in their interactions. For instance, moderator vaccine status, wearing a mask and conducting the interview outdoors may be important factors for certain patients. As always, you must ensure there are proper consents in place prior to the interview and that the moderator is aware of all the requirements. For example, depending on the condition and its severity, some patients will opt out of webcam interviews and it is essential for the moderator to know this beforehand to avoid beginning the interview with the expectation that the patient will be seen on screen or putting pressure on the patient to do so.
Good moderators know that questions should not be leading and should be appropriate for the patient type. In the case of rare disease patients, every interview is crucial, so you should make sure questioning is relevant for the condition and to the specific patient. The discussion guide should be considered just that – a guide – and the moderator should be empowered to go off-script to tailor the discussion.
One way to do that is to review any pre-task activities done by the respondent. The pre-task activities provide a more holistic understanding of the patient disease experience, allowing the patient to describe their condition and its impact in their own terms and in their own time. In a pre-task, the patient provides information about their background and experience, which can be in a written, audio or video format. Pre-tasks are a very individualized activity and generally tend to focus on the milestones that are important to them.
When trying to elicit emotional or less consciously available thoughts, projective techniques can be useful. Projective techniques are used as mechanisms for bringing to the surface feelings and associations that are not immediately conscious. The principle of projection is that people can give voice to underlying feelings by projecting them onto someone or something else. The principle of enabling is that people are provided with mechanisms that help them express thoughts, ideas or emotions where language is not readily available or where these have not been previously consciously thought about. They are designed to give people ways of accessing, structuring and expressing/articulating thoughts and feelings. This is especially crucial in patient research. Many key milestones in journeys, such as receiving a diagnosis, may be difficult to recall or speak about. Children may find it challenging to articulate their thoughts and perceptions towards their condition. Projective techniques can aid in overcoming some of those barriers.
Approaches to analysis
During the research, there are different types of data that may be collected. Moderators make specific observations and provide ratings based on their perception. This is often done live during the interview using a moderator sheet, as well as afterwards upon reviewing the recordings. For device-testing research, observational analysis is even more important than traditional probing typically used in qualitative research; for example, the respondent might say the device is very easy to use but may actually appear to be fumbling with it or perform the procedure incorrectly. There also may be a knowledge task for the respondents that would allow us to capture this after they have learned a new procedure. Respondents can provide qualitative feedback and ratings on specific metrics during the interview. All of this information can be included in the analysis and reporting (see Figure 3).
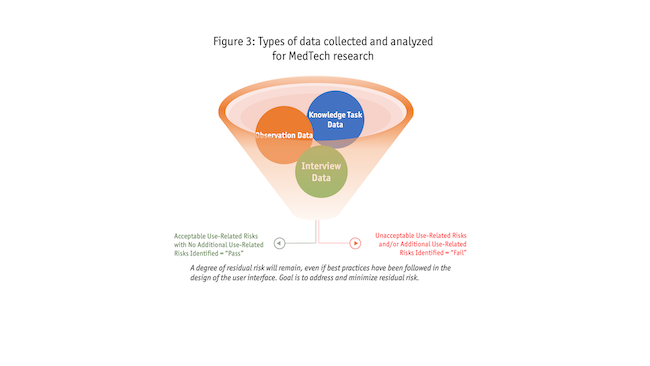 Consider whether analyses should be done separately by type of respondent or method, because some approaches may be given more weight (e.g., in person hands-on usability vs. virtual interviews with images). In typical qualitative marketing research, we tend to avoid counts and use terms such as many, some and few. However, in device research, human factors engineers require specific numbers. When use of a device is observed, the frequency of behaviors that deviate from the appropriate use is reported. These all help the research team determine user needs, potential design updates and whether the use-related risks are acceptable. In the case of rare-disease patients, your sample size will be small, particularly within a given method and respondent configuration type.
Consider whether analyses should be done separately by type of respondent or method, because some approaches may be given more weight (e.g., in person hands-on usability vs. virtual interviews with images). In typical qualitative marketing research, we tend to avoid counts and use terms such as many, some and few. However, in device research, human factors engineers require specific numbers. When use of a device is observed, the frequency of behaviors that deviate from the appropriate use is reported. These all help the research team determine user needs, potential design updates and whether the use-related risks are acceptable. In the case of rare-disease patients, your sample size will be small, particularly within a given method and respondent configuration type.
The approach to reporting with patients is often very different from reporting marketing research with health care professionals. Typically, patient reports incorporate both the rational and emotional insights to capture patients’ daily lives with their condition. As mentioned previously, each rare-disease patient journey is extremely individualized. Therefore, it may make sense not to aggregate findings and to create individual stories for each patient as silhouettes or spotlights, for example. Often, the smaller sample sizes that encompass rare-disease research, as mentioned previously, enable us to do so.
Deliverables are also very customized per project; creative deliverables outside of the standard PowerPoint report are often a nice supplement to the research. The nature of the pre-tasks or the interview itself may support the creation of interactive deliverables, such as a video or interactive patient journey link. This aids in bringing the patient journey to life.
Flexibility required
MedTech research with rare-disease patients requires flexibility on the part of everyone involved to achieve study objectives: the respondents, recruiters, moderators and clients. The methodology and recruitment must be flexible, allowing a combination of in-person interviews in a facility, in-home interviews and virtual interviews. A combination of interviewing patients and/or their caregivers should be considered. Our hybrid approach to MedTech research with rare-disease patients has proved effective across a range of studies. Respondents and clients appreciate a flexible approach because it captures the study objectives while fitting into patients’ real-life needs and the reality of the rarity of the disease.
References
1 https://www.fda.gov/patients/rare-diseases-fda
2 https://emmes.com/orphan-and-rare-disease-research
4 https://rarediseases.info.nih.gov/diseases/6468/friedreich-ataxia
5 https://www.hopkinsmedicine.org/health/conditions-and-diseases/friedreich-ataxia
6 https://rarediseases.info.nih.gov/diseases/7674/spinal-muscular-atrophy
7 https://rarediseases.info.nih.gov/diseases/7674/spinal-muscular-atrophy
8 https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-muscular-atrophy-sma