An incomplete diagnosis
Low health literacy is related to medication errors, device misuse, lower compliance and poor health but is traditionally not considered in marketing research studies. Based on studies conducted by members of the Pharmaceutical Marketing Research Group’s Health Literacy Initiative committee, this article aims to raise awareness of how health literacy could be used as a lever to improve public health, while challenging marketing researchers to consider health literacy as both a responsibility and an opportunity in their research designs.
The Pharmaceutical Marketing Research Group (PMRG) is an independent, non-profit trade association whose purpose is to stimulate the advancement of marketing research in the health care industry. PMRG serves U.S. and global end-client researchers and service providers representing pharmaceuticals, biologics, medical/surgical device and diagnostics.
The PMRG Health Literacy Initiative (HLI) provides leaders in health care marketing research with the tools and understanding required to address the needs of all patients. It is a collaboration of members across the health care industry including manufacturers, payers and agency organizations. By providing education, resources and training, the PMRG HLI works to drive change within our industry and at the FDA. This change will ultimately reach and empower patients to take control of their own health and to better understand their conditions and treatments.
This article presents: evidence of the negative impact of low health literacy on compliance; the challenge low health literacy presents to marketing research; results from two marketing research studies, one with health care practitioners, the other with patients; and an outline of marketing researchers’ responsibility and opportunity.
Well-being suffers
Patients’ well-being suffers with poor understanding of their health and available treatments. Device and medication misuse can cause problems for patients’ health. In fact, poor health literacy is “a stronger predictor of a person’s health than age, income, employment status, education level and race.”1
Consider the following:
- In the U.S., 3.8 billion prescriptions are written every year. More than half of those prescriptions, however, are taken incorrectly or not at all.2
- In a survey of 1,000 patients, nearly 75 percent admitted to not always taking their medications as directed.3
- A study of over 75,000 commercially-insured patients found that 30 percent failed to fill a new prescription.4
- It’s estimated that poor compliance costs the U.S. health care system $290 billion each year.5
There are many explanations of what leads to medication errors, device misuse and lower compliance. Although the high cost of medications is often referenced as a major reason for poor adherence, compliance rates improve only marginally when the cost barrier is removed. With an aging population, there has been an increase in the number of medications – with different dosing schedules – given to individual patients to treat a variety of chronic medical conditions. This can lead to confusion over treatment schedules. There can also be contraindications among various medications resulting in unintended side effects or other problems affecting adherence to a prescribed plan.
In 2009, Kaiser Permanente conducted an exhaustive literature review on the topic of non-compliance and found seven patient-related barriers to compliance:6 forgetfulness; financial challenges; lack of knowledge about the medication and its use; lack of social support; cultural, health and/or religious beliefs about the medication; lack of health literacy; and denial or ambivalence regarding the state of their health.
Studies suggest a link
The key to understanding and improving compliance is the role of health literacy, which has been defined as “the degree to which individuals have the capacity to obtain, process, understand, [and act upon] basic health information and services needed to make appropriate health decisions.”7 Multiple studies suggest a link between low health literacy and low comprehension.
Research shows only 12 percent of the population is health literate.8 People with low health literacy may not understand their health issues (e.g., diabetes, high blood pressure, high cholesterol). This lack of understanding can result in devaluing its treatment, which can negatively impact their health in the long term.
While certain populations are at greater risk for experiencing limitations on their health literacy (e.g., individuals who speak English as a second language), the state is by no means static. Rather, health literacy is dynamic, changing for individuals based on the context of any given situation. Even people with advanced education and reading skills can face health literacy challenges. Consider the stresses imposed by health emergencies. At such times, even the most health-literate individual may experience difficulties understanding or processing health information. Simpler and easier-to-understand patient materials, therefore, benefit everyone.
Those with limited health literacy are less likely to understand terminology, risks and benefits9,10 and lower health literacy has been linked to poorer overall health outcomes – higher rates of hospitalization than in individuals with higher health literacy11,12,13 and higher mortality rates than in individuals with higher health literacy.14 And though the link is not definitive, the relationship between health literacy and outcomes likely reflects inadequate self-care behaviors.
Many factors affect a person’s health literacy, including their reading ability, age, culture, the complexity of the information presented and language skills.15 Some population groups are particularly vulnerable to health literacy challenges: adults age 65 and over; those who don’t understand or speak English well; minorities; and low-income populations.16
Main challenges for researchers
For marketing researchers, there are four main challenges that low health literacy presents:
Recruitment. Patients with low health literacy are traditionally screened out of samples because researchers want respondents who can understand the information provided in the study and can effectively communicate their feedback. This common practice leads to the exclusion of an important segment of the population. When the study has implications for communications to patients, such as patient education materials or instructions on using a device, this approach is deficient in research design and also doesn’t allow for the learnings that will help create materials that can be better and more easily understood. It is difficult to recruit people with low health literacy and the tools are still being developed for properly screening for health literacy. While the Newest Vital Sign (NVS) tool (one we recommend for identifying people with low health literacy) has been validated for in-person research, it has not yet been validated for online research.
Participation. Patients who are lower in health literacy tend to be more reluctant to participate and voice their opinions. This lack of participation arises from lower confidence or embarrassment in their abilities, such as having difficulties speaking, reading and/or understanding – whether it is a challenge with the English language or medical terminology. Researchers must change the way they collect their data in order to make this work. For example, during in-person research, moderators should provide extended warm-up time at the beginning of the interview to build trust. They should also understand that bland or non-committal participation (e.g., “Yes, I agree” or “No, I do not like that”) are a signal of potential problems and thus be prepared to shift activities as needed to get more-involved participation and better data.
Analysis. Once included into the research, data for low health literacy patients should be analyzed separately from those with adequate literacy to ensure the needs of this at-risk group are not missed. With the proper data collection techniques, researchers should have uncovered the true reactions of the low health literacy group to be included in consideration, rather than being lost in background noise.
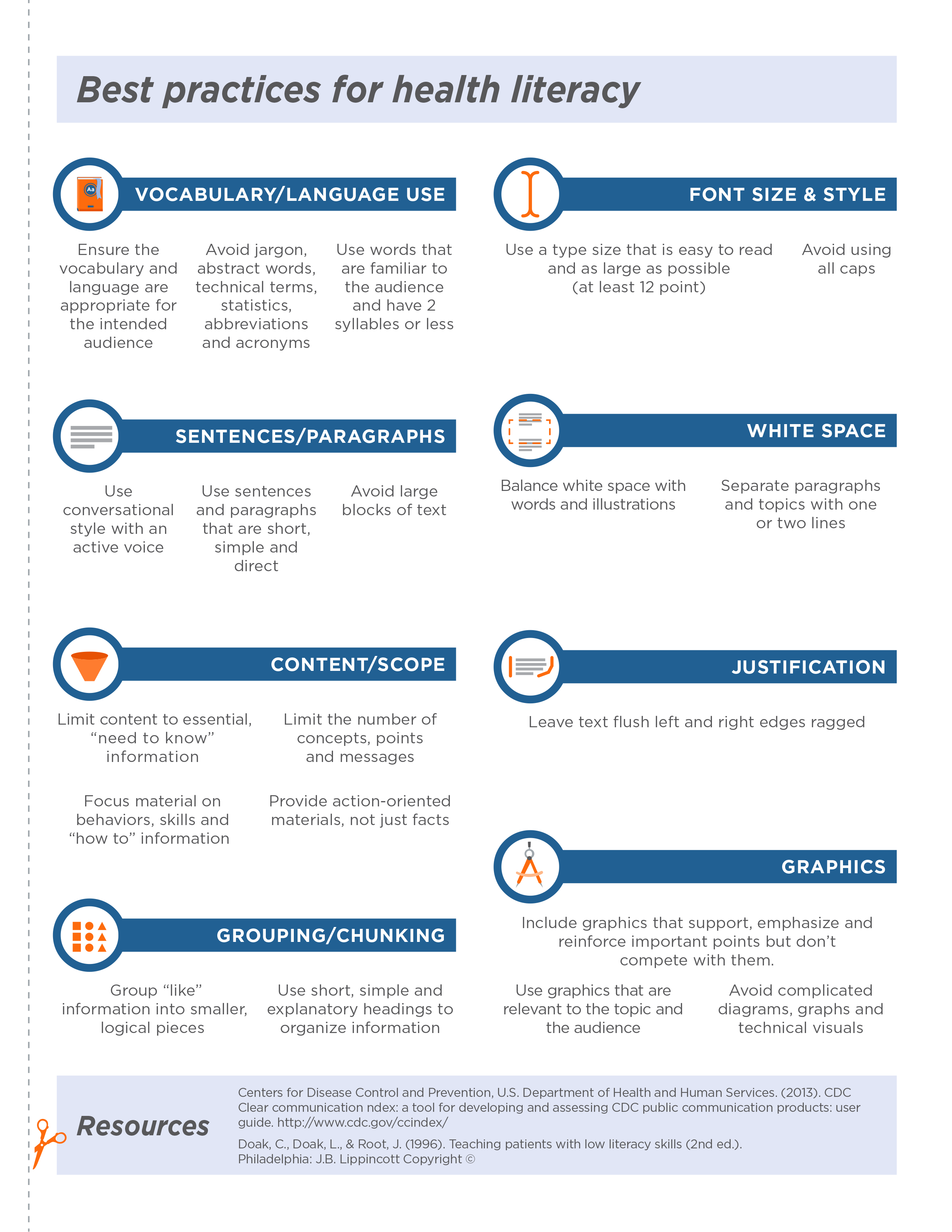
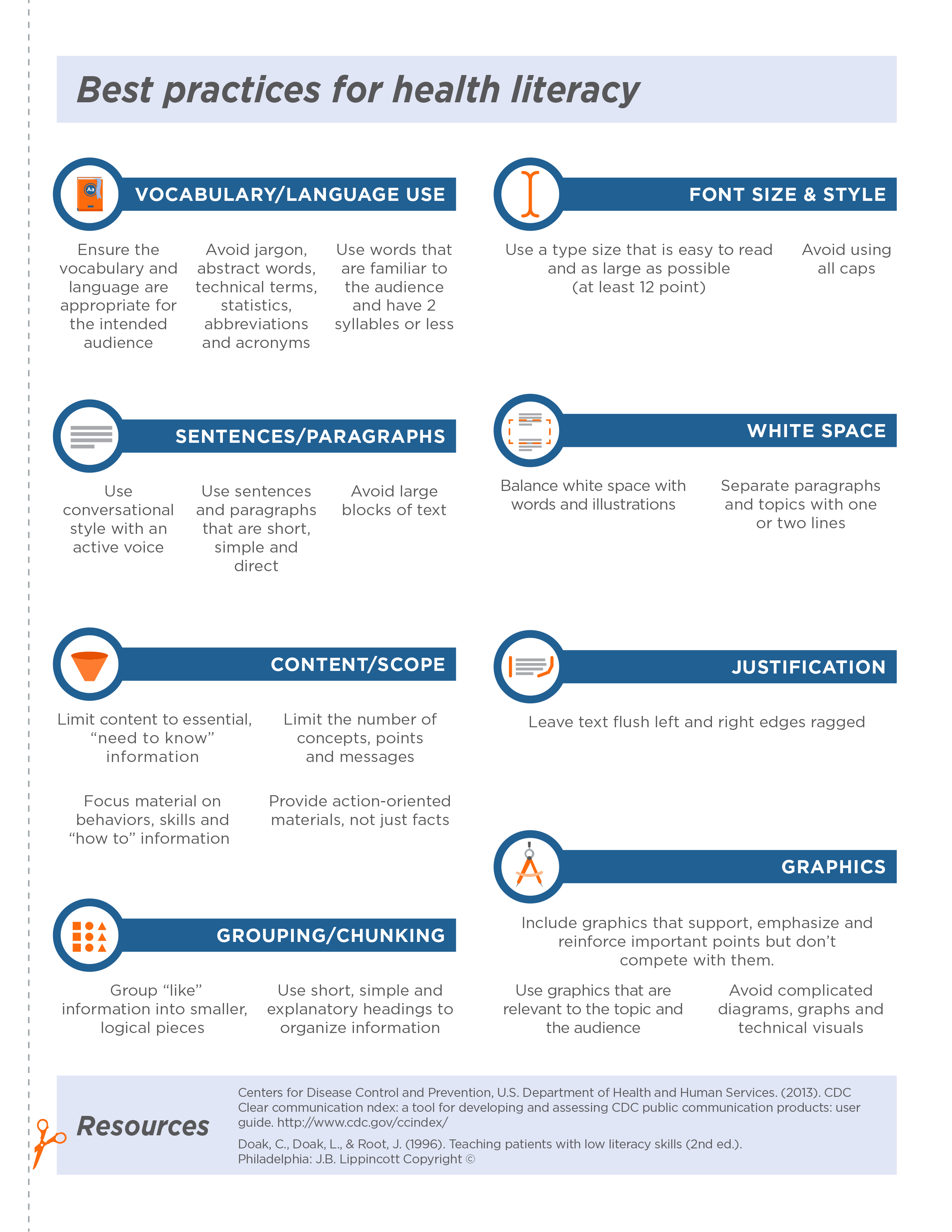
Stimuli. The stimuli used in research – which are often closely linked to the actual communication to the patients – should be formatted to follow best practices for health literacy. Some of those best practices include (see the graphic below for a more complete list):
- avoiding jargon, abstract words, technical terms, statistics, abbreviations and acronyms;
- using a type size that is easy to read and as large as possible (at least 12-point text);
- using sentences and paragraphs that are short, simple and direct;
- providing action-oriented materials, not just facts;
- grouping related information into smaller, logical pieces;
- avoiding complicated diagrams, graphs or technical visuals.
To better understand how marketing research may be affected by the challenges of low health literacy and to quantify the impact that utilization of health literacy best practices may have in marketing research, the HLI Committee conducted two marketing research studies, one with health care practitioners and another with patients. As noted above, special efforts were taken to include low health literacy patients who are not usually included in traditional market research studies.
Health care practitioner study
Sample and method. Conducted by Doctor Directory. Physicians (n=100) and pharmacists (n=50) were asked in an online 10-minute survey about compliance and communication with their high blood pressure (hypertension) patients.
Key findings. In terms of compliance, there is a disconnect between the physicians and the pharmacists. From the physician perspective, most of their patients with high blood pressure understand their prescription instructions and are taking their medication as prescribed.
Physicians believe: 78 percent of patients are taking their medication as prescribed and 88 percent understand how to take their medication.
Pharmacists provide a less-optimistic patient compliance story. Most pharmacists say: up to 24 percent of hypertensive prescriptions are abandoned; up to 24 percent of initial starts are not refilled; and up to 49 percent are refilled late.
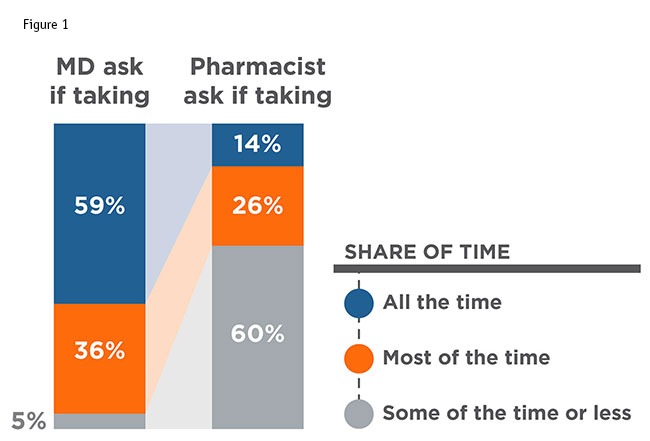
This gap between the perceptions of physicians and pharmacists on patient compliance is concerning and there is no formal process connecting physicians and pharmacists to allow feedback on medication compliance. In terms of communication with the patients, doctors and pharmacists have two different roles. Doctors are focused more on telling patients how to dose and asking if they are taking their medication during follow-up visits when they occur, while pharmacists are not directly asking if patients are taking their medication (Figure 1). There is a gap in care between the roles of physician and pharmacist that widens with low health literacy.
Physicians and pharmacists agree that between 15 and 20 percent of patients have hearing difficulties or difficulties with understanding or reading English.
Health literacy is not mentioned when physicians are probed as to what triggers them to ask compliance questions of patients (Figure 2). This is the case despite physicians recognizing that some of their patients may experience communication challenges (e.g., hearing difficulties, limited ability to read and/or understand English, etc.).
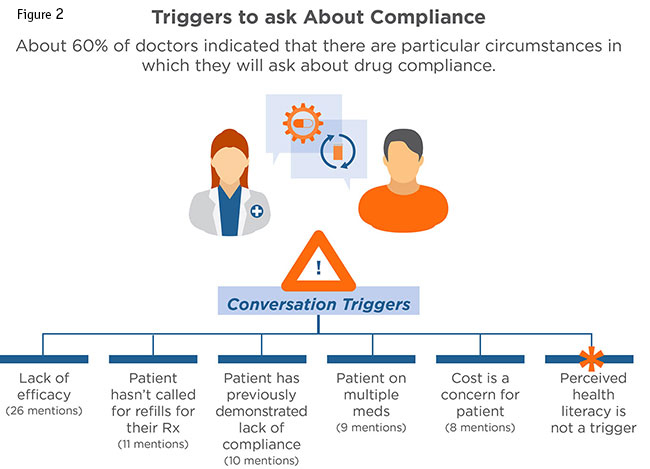
None of the mentioned triggers validate if a patient understands their diagnosed condition or the short- and long-term benefits of their treatment.
As we see in the above research, noncompliance may be worse than physicians are aware because there is no formal feedback for when a patient fills, takes or stops taking a medication. There is no understanding of why a patient doesn’t start or stops taking a medication. Without feedback, no follow-up conversations can occur nor can education on the condition, benefits of treatment or safety concerns be addressed.
Patient study
For the patient study, the objectives were to: assess individuals’ health literacy; assess comfort with filling out medical forms; and determine how an individual’s health literacy impacts their ability to read a medication label.
Sample. Fielded by MarketVision Research. Research was conducted with 805 patients, half of whom had high blood pressure and half among the general population. Special recruitment was in place to ensure adequate numbers of patients with low income and low education. Respondents completed a 10-minute online survey.
Method. Although the Newest Vital Sign has only been validated for in-person research, we adapted the tool for online use. A component of this research was used to understand how the NVS may be administered online. The measure used was a series of six questions about an ice cream nutrition label. Respondents were grouped into adequate vs. limited health literacy based on their score. Later in the survey, respondents were given a series of five questions about a drug label. Half of each group was randomly given the traditional label and half was randomly given the optimized label.
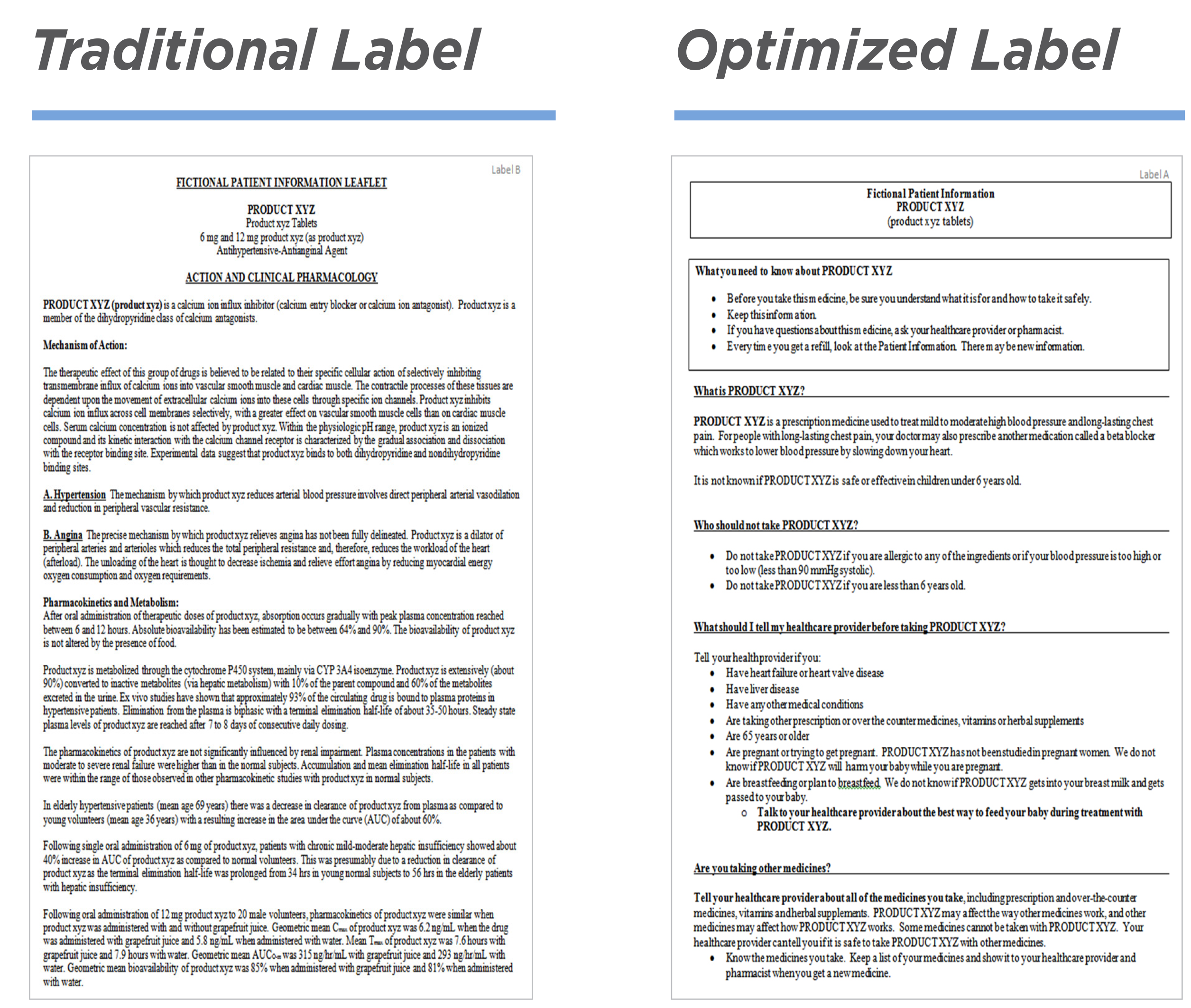
Stimuli. For the purposes of this study, the traditional pharmaceutical label was modified into the optimized label by following some of the health literacy best practices described above. (See below for examples of the traditional and optimized labels.) This was a proof-of-concept study, to allow us to document the effect a minimum change would have. If this were an actual marketing research study for a product to be launched, we would recommend engaging a health literacy consultant and conducting research with people who have low health literacy.
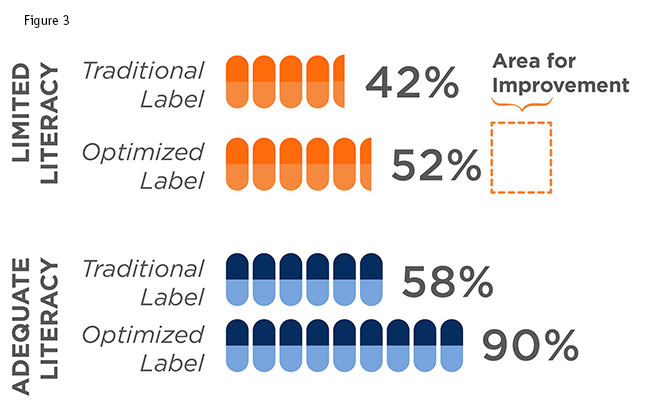
Key findings. Contrary to expectations, the improved label did not have a big effect among those with low health literacy, with only slightly improved comprehension of the product label (Figure 3). This highlights the importance of additional work such as including low health literacy respondents in research and hiring a health literacy consultant to achieve a better result for this group. Most surprising to us, the biggest positive effect on comprehension was seen among those who had adequate health literacy. The comprehension level was raised by over 30 percent, to a level indicating that almost everyone with adequate health literacy understood the basics about the drug. This illustrates a side benefit of including those with low health literacy in our research – that by doing so we will improve comprehension for all.
This patient study shows the need to: include low health literacy patients in the sample design; separately analyze performance of low health literacy patients; and carefully craft patient communications using best practices and expert consultation.
Key lever
Health literacy can be a key lever in improving patients’ health. With some simple techniques, comprehension can increase, which could lead to improved compliance, as well as reduced medication errors and device misuse.
As discussed, there are four challenges that low health literacy presents to marketing research.
Recruitment: Are special efforts used to include patients with low health literacy in the sample?
Participation: Are special techniques used to gain their true reactions?
Analysis: Are their results scrutinized vs. dismissed as background noise?
Stimuli: Were the tested materials formatted optimally?
As researchers, we are responsible for the proper design, execution and analysis of our studies. The research may be flawed if patients with low health literacy are not considered.
Beyond your responsibilities as a marketing researcher, consider your opportunity to provide added value to your client, as well as your client’s client. Armed with the above knowledge, you are empowered to help move the industry towards better market research and, ultimately, higher levels of patient health.
References
1 Parker, R., et al. “Library outreach: overcoming health literacy challenges.” Journal of the Medical Library Association. 2005 October; 93 (4 Suppl): S81-S85.
2 Cutler, D.M., Everett, W. “Thinking outside the pillbox – medication adherence as a priority for health care reform.” New England Journal of Medicine. (2010). 362:1553-1555.
3 Osterberg L., Blaschke, T. “Adherence to medication.” New England Journal of Medicine. (2005) 353:487-489.
4 “Enhancing prescription medication adherence: a national action plan.” National Council on Patient Information and Education. August 2007.
5 Fischer, M.A., Stedman, M.R., Lii, J., et al. “Primary medication nonadherence: analysis of 195,930 electronic prescriptions.” Journal of General Internal Medicine. (2010) 25:284-290.
6 Oyekan, E., Nimalasuriya, A., Martin, J., et al. “The B-SMART appropriate medication-use process: a guide for clinicians to help patients – part 1: barriers, solutions, and motivation.” The Permanente Journal (2009) 13:62-69.
7 U.S. Department of Health and Human Services. Healthy People 2010. Washington, D.C.: U.S. Government Printing Office. 2000.
8 U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. www.health.gov/communication/literacy/issuebrief/. Accessed on 11/12/13.
9 Russell, Michael J.M., Mullan, Judy, and Billington, Timothy. “Health literacy and patient comprehension in the pre-anaesthetics consultation.” Australian Medical Student Journal. (2015) 6(1).
10 Donovan-Kicken, E., Mackert, M., Guinn, T., Tollison, A., Breckinridge, B., and Pont, S. “Health literacy, self-efficacy, and patients’ assessment of medical disclosure and consent documentation.” Health Communication. (2012) 27: 581-590.
11 Baker, D.W., Parker, M.R., Williams, M.V., and Clark, S.C. “Health literacy and the risk of hospital admission.” Journal of General Internal Medicine. (1998) 13(12): 791-798.
12 DeWalt, D.A., Berkman, N.D., Sheridan, S., Lohr, K.N., and Pignone, M.P. “Literacy and health outcomes: A systematic review of the literature.” Journal of General Internal Medicine. (2004) 19: 1228-1239.
13 Wolf, M.S., Gazmararian, J.A., and Baker, D.W. “Health literacy and functional health status among older adults.” Archives of Internal Medicine. (2005) 165: 1946-1952.
14 Baker, D.W., Wolf, M.S., Feinglass, J., Thompson, J.A., Gazmararian, J., and Huang, J. “Health literacy and mortality among elder persons.” Archives of Internal Medicine. (2007) 167: 1503-1509.
15 U.S. Department of Health and Human Services. Office of Disease Prevention and Health Promotion. National Action Plan to Improve Health Literacy. Washington, D.C.: 2010.
16 Weiss, B.D. Health Literacy and Patient Safety: Help Patients Understand. American Medical Association Foundation and American Medical Association. May 2007.