
A healthy dialogue
Editor's note: Tom Donnelly is senior vice president of iMarketResearch. He can be reached at tom.donnelly@thinkimr.com. Vincent Valant is product manager at ZoomRx. He can be reached at vincent.valant@zoomrx.com. Barbara Haimowitz is president of The DataMine Inc. She can be reached at barbanalysis1@gmail.com. Derek McCracken is co-founder of Narrative Mindworks. He can be reached at derek.mccracken@narrativemindworks.org. Sara Bell is senior manager at ZoomRx. She can be reached at sara.bell@zoomrx.com. Julie Leonard is vice president of qualitative research at MarketVision Research. She can be reached at jleonard@marketvisionresearch.com. Peter Simpson is managing partner at Sarasota Ventures. He can be reached at peter.simpson@sarasotaventures.com. The authors would like to thank ZoomRx for access to these HCP-patient dialogues. This project was funded by Intellus Worldwide, a not-for-profit organization dedicated to advancing the field of health care insights and analytics.
The medical appointment is where marketing to the health care provider (HCP) meets direct-to-consumer marketing, as well as where key health care decisions are made. Understanding the dynamics of these interactions is critical to meeting brand objectives and improving patient health outcomes. It is widely recognized that there is room for improvement in these conversations. (October has marked Health Literacy Month since 1999.) How might they be improved? How can health care manufacturers and insights professionals help?
In this article, we present several vignettes that include unique, de-identified patients with varied disease states in conversation with different types of HCPs. We show some of the pitfalls and roadblocks HCPs and patients can encounter in conversations that make it harder to connect with and understand each other and decide on the final direction for future care. This triple threat may have repercussions for patient health outcomes and hinder treatment progress. This article also amplifies the role of the translator, the importance of staying close to what is being said in the dialogue to avoid misinterpretations and speaking out of turn.
Outcomes are more successful
During a dialogue with a patient, it is critically important for the HCP to fully comprehend the patient’s perspective and ensure that any information shared is clear, relevant and tailored to the patient’s ability to understand and use it effectively. When conversations have a foundation in clear health communication (CHC) principles, comprehension and patient outcomes are more successful. Strong CHC practice includes using everyday words, short sentences, simple visuals and teach-back techniques.
In our foundational research,1 we validated that refining written resources (e.g., booklets, patient package inserts, flyers, etc.) with CHC best practices improves comprehension for individuals at all levels of health literacy. This means providing a basic explanation at a uniform level to all patients initially rather than attempting to tailor the information based on assumptions of a given patient’s health literacy level.
This is confirmed in our follow-up study,2 in which we found that HCPs are often inaccurate in identifying the health literacy levels of their patients. The need for CHC is important in the typical medical office setting but is even more important in the emergency room (ER). This is especially relevant for patients with limited English proficiency. In our recent research,3 we found that it takes about 11 minutes until language assistance arrives for these patients. That is much too long for an urgent situation in the ER. Even more alarming is that the wait time increases to almost 45 minutes in low-resource areas (commonly faced with high levels of health disparities). Outside the ER, natural language processing has been used to detect patient-spoken language in home health settings, potentially translatable to ER documentation.4
Using CHC approaches ensures that the HCP-patient dialogue is effective, that their limited time together is well-spent and that patients and HCPs understand each other. This collective success bridges language barriers, increases patient adherence and ultimately improves patient health and satisfaction with their health care experience. This need conflicts with the fact that providers are trained to use precise and often Latin-based language, as well as to maintain a professional distance between themselves and patients. This training can conflict with the process of establishing rapport, building trust and making emotional connections with patients. Clear health communications help providers step outside of this traditional training and connect with patients on a different level. This co-created approach is exactly what is needed to change the narrative.
What are the characteristics of an impactful dialogue?
- The patient feels understood, heard and believed in their description of symptoms.
- The HCP is clear and believable in their analysis of the patient's concerns.
- The HCP provides reasons why the patient should begin a treatment plan, stay on the current treatment path or change to another path that is perceived as more efficacious.
- When a patient feels the HCP has their best interests in mind, they place greater trust in subsequent follow-up steps. If this sense of trust is absent, the patient is less likely to come to a consensus with the HCP or adhere to treatment recommendations.
Different types of conversations between an HCP and patient demand unique adaptations to achieve ideal outcomes. To support the health care industry in improving future HCP-patient dialogues, it is important to examine real-world conversations and offer potential optimizations to meet these adaptation needs.
Learning from HCP-patient dialogues
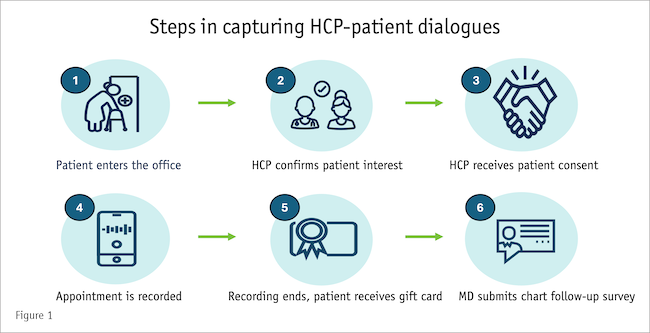
Our capturing of HCP-patient dialogue includes several steps to ensure the research follows and adheres to industry guidelines and local laws (see Figure 1, courtesy of ZoomRx). When the patient arrives at the health care site, they are asked if they are interested in participating in the research. If so, the appropriate consent forms are reviewed and signed. The dialogue is recorded, the patient is provided with an incentive (not a direct payment) and the recording and other anonymized patient chart information is shared with the research agency.
HCP-patient dialogue research offers an insight-provoking format that provides several unique benefits: it allows researchers to better understand the patient experience through the words that they use; it shows how patients articulate what is most important to them; it uncovers how HCPs engage with patients in the exam room and identifies what information is shared and how patients engage in the discussion.
While reviewing such dialogues, researchers should consider: What is clear or unclear about the communication? How are the specific word choices of HCPs and patients aligned (or misaligned)? What is communicated well? What elements could be improved?
Three HCP-patient dialogues were analyzed through a CHC lens to provide suggestions for pharmaceutical manufacturers, health care practitioners and insights agencies. In particular, the examples highlight: open- vs. closed-ended questions; probing questions that require a creative, engaging response; and challenges inherent to translated conversations.
Dialogue 1: Prostate cancer patient
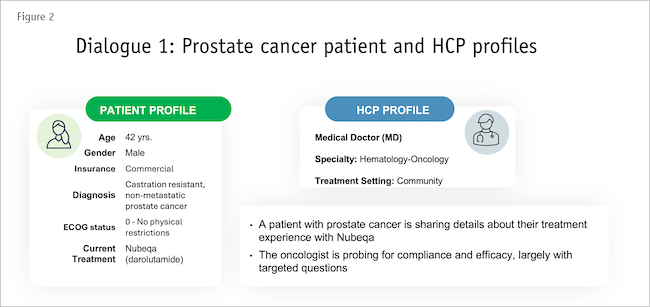
This first example conversation is from a prostate cancer appointment with a 42-year-old patient sharing details about their treatment experience with Nubeqa (see Figure 2 for details about the HCP and patient). The hematologist-oncologist is having a check-in with their patient after starting their first treatment, probing for compliance and efficacy, largely with targeted questions.
MD: The reason why we chose darolutamide is because you are a very young patient and you are still working full-time, of course, and you wanted to have a treatment which would not cause too much fatigue or cognitive dysfunction. How have you been doing with the darolutamide? How do you take it?
Patient: I don't have any problems.
MD: Do you take it after food?
Patient: I do not feel anything.
MD: Do you take it after food? I'm just checking to make sure that, you know, you're taking it correctly.
Patient: Yes, that's what I do.
MD: Ok. And you're taking it twice a day?
Patient: Yes, uh huh, just like you told me.
MD: Ok, so I'm just checking because some patients take it on an empty stomach. So you have to take it with food. So you're saying that you have not noticed any side effects so far?
Patient: No, no.
MD: Okay, that's amazing. That's very good, that's very, very good. So are you able to concentrate, you know, as usual and work as usual?
Patient: Yes.
MD: Do you feel tired or no?
Patient: Not really, I feel better. I feel like I have more energy.
MD: You feel better? Oh, Okay.
The team’s analysis
The HCP shares the context behind his questioning and normalizes any patient-made mistakes such as forgetting to take it with food. He then goes on to relate potential side effects to what he knows about the patient. The HCP continues to use closed-ended questions for most of this discussion but was able to get the patient to open up. Notice that the HCP is quite interrogative and it is possible that continued probing on the same point may feel pushy to a patient. In addition, the HCP makes assumptions that were more difficult to objectively verify, such as asking about his ability to concentrate at work.
Looking at the patient’s part of the conversation, the patient does not give the HCP much to work with, saying “I don’t have any problems,” which closes the conversation off. This could have been an opportunity for the HCP to insert some broader and open-ended questions such as “Describe for me how and when you’re taking the medication.” While this may seem challenging given typically short appointment times, the HCP could likely have elicited more detail in a shorter time with open questions and better understood the patient’s experiences.
Dialogue 2: Psoriasis patient
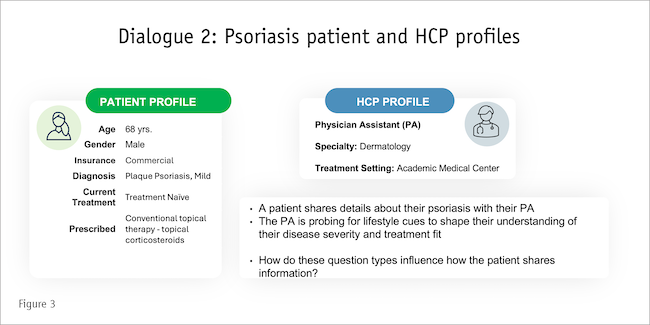
The second conversation features a 68-year-old male with psoriasis (treatment-naïve), meeting with a physician assistant (see Figure 3 for details about the HCP and patient).
Physician assistant (PA): So, tell me what bothers you about your psoriasis? I see it on your head, do you have it anywhere else?
Patient: Yeah, it's really bad on the head right now if you look. And then, if you look at my nails on my hands, you can see it on both hands. It's just bothering the heck out of me.
PA: Okay. Have you tried anything? Does the doctor give you anything to put on it?
Patient: They tried to put me on some oral medication that works in my whole body but I'm not a big fan of that.
PA: I understand. Do you have any stiffness in your hands? I see the nails here as I'm looking, do you have any stiffness when you wake up in the morning?
Patient: Yeah, a little bit.
PA: Does it last more than an hour or less than an hour?
Patient: Less than an hour.
PA: Once you get moving, it's okay?
Patient: Yeah, definitely.
PA: Okay. Tell me about the shampoo that you have used for your scalp, has anything helped?
Patient: Not so much, but you know what I want to ask you like you could suggest any creams or anything that I could use. I really don't want to get on more pills at this point in my life.
PA: I understand.
The team’s analysis
Immediately, the PA starts with open-ended questions to get a sense of what the patient is experiencing. After that, however, the PA uses closed-ended questions to obtain targeted information before reversing course and opening up the conversation to ask about past treatments. The PA’s questions are mostly surface-oriented, asked in rapid-fire sequence and related to history-taking. There are opportunities for the PA to utilize more observational techniques and to probe more in-depth into the patient’s experiences and to gain understanding of the patient’s hesitation to use oral medication to treat. The patient, ultimately, does not get their needs met; the PA offers no solution.
Dialogue 3: HIV patient with an interpreter
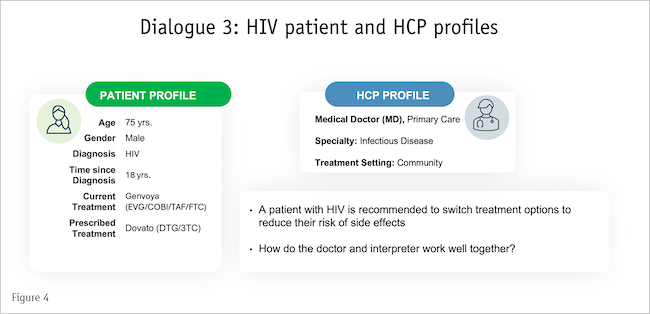
In the third example, there is a three-way conversation involving an HCP, an interpreter and a patient. This conversation captures a discussion with a 75-year-old non-English-speaking patient who has had HIV for 18 years (see Figure 4 for details about the HCP and patient). The patient has been treated with Genvoya for a while and is having a regular check-in with his HCP. Given the complexity of the dialogue, we break it into four parts.
Part 1: Interpreter creates their own question and HCP intercepts
The team’s analysis
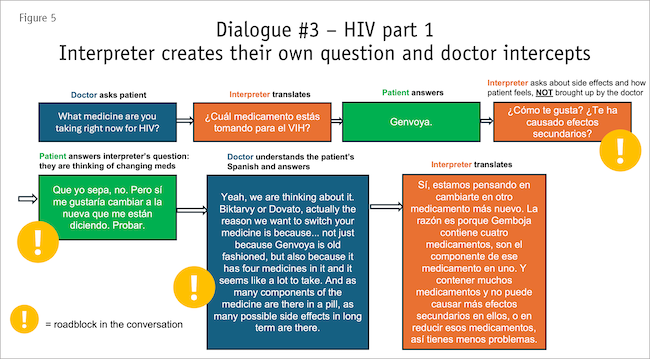 In this conversation (Figure 5), the HCP introduces a few new treatment options and explains the rationale for suggesting a switch. The interpreter does a good job at capturing most of the context without modifying it much and the HCP does well to pause frequently enough to allow the conversation to flow appropriately. The conversation is significantly slower than the other two HCP-patient dialogue examples (and takes twice as long to cover the same amount of information). The HCP also does well, pausing at the end of each segment and checking in with the patient. However, there are some areas where one of the parties in the conversation creates a roadblock. For example, the interpreter asks about side effects and how the patient feels, which is not initiated by the HCP; consequently, the patient answers the interpreter’s question. The HCP understands the Spanish and intercepts the discussion.
In this conversation (Figure 5), the HCP introduces a few new treatment options and explains the rationale for suggesting a switch. The interpreter does a good job at capturing most of the context without modifying it much and the HCP does well to pause frequently enough to allow the conversation to flow appropriately. The conversation is significantly slower than the other two HCP-patient dialogue examples (and takes twice as long to cover the same amount of information). The HCP also does well, pausing at the end of each segment and checking in with the patient. However, there are some areas where one of the parties in the conversation creates a roadblock. For example, the interpreter asks about side effects and how the patient feels, which is not initiated by the HCP; consequently, the patient answers the interpreter’s question. The HCP understands the Spanish and intercepts the discussion.
Part 2: Presentation and interpretation in small information chunks
The team’s analysis
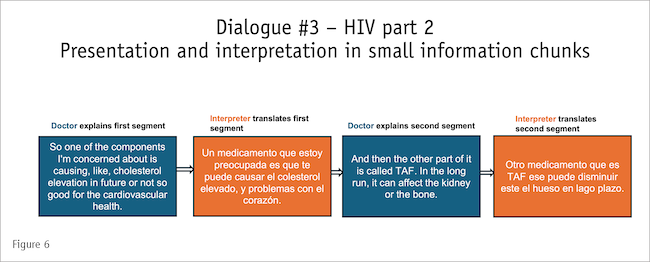
This approach (Figure 6) is great for working with an interpreter. It provides small information snippets (“chunking”). However, chunks that are too big are often not shared word-for-word, not always translated properly and thus are not effective.
Part 3: Patient doesn’t understand and interpreter translates incorrectly
The team’s analysis
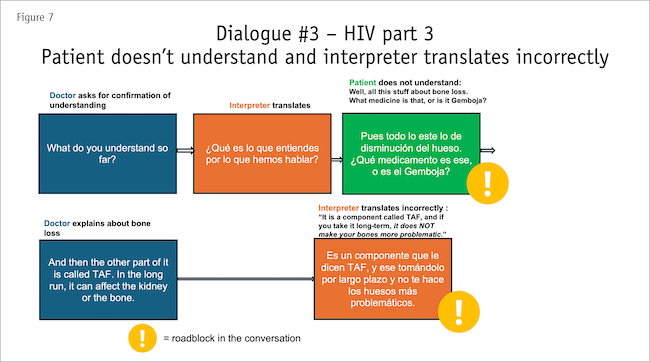
This (Figure 7) is a quintessential example of an HCP effectively using teach-back (“What do you understand so far?”). Since the patient does not understand the bone loss component associated with the drug, the HCP explains it in more detail; however, the interpreter translates the HCP’s comments incorrectly.
Part 4: HCP translates on their own
The team’s analysis
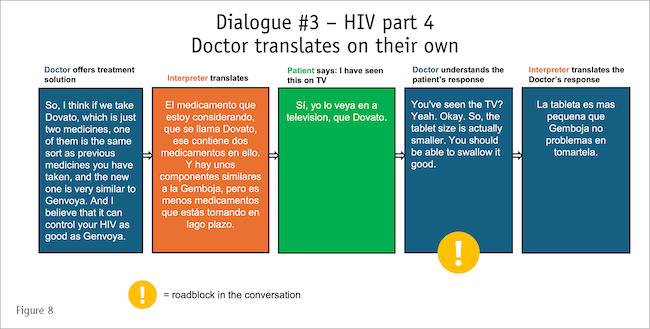
Because the HCP understands Spanish (Figure 8), they translate the patient’s response on their own, with the interpreter then translating the HCP’s response.
Recommendations
In a health care setting, time is limited, urgent and chronic issues are presented and the patient’s emotional state may be heightened. Meanwhile, the HCP needs to be calm, clear and decisive. To achieve the best health care outcomes, the HCP-patient dialogue should:
- Use broader, open-ended questions strategically.
- Avoid using surface-oriented, closed-ended questions that can come across as a rapid-fire approach to capturing patient history.
- Use probing questions that invite a detailed, engaging response from the patient.
- Use observational techniques to aid in deeper probing.
- Use teach-back methods to ensure the patient’s understanding.
- When working with an interpreter, “chunk” information into smaller communication building blocks so that the three-way conversation is clear and reflects what the patient and HCP are trying to convey, with a clear endpoint in mind that results in optimal understanding of the situation and next steps for treatment.
Enhance the impact
Based on our research in health literacy and the HCP-patient dialogue, we have suggestions for the health care industry to help enhance the impact of the HCP-patient dialogue.
Health care providers
- Make efforts to see the whole person and meet them where they are physically/emotionally/mentally.
- Consider the patient journey pain points and touchpoints.
- Use open-ended and probing questions to elicit deeper sharing.
- Practice “teach-back/show me” techniques to confirm full comprehension
Pharmaceutical manufacturers
- Lead the industry promoting the use of CHC principles across all health communications including product advertising/marketing messages, clinical trial communications and in sales force training.
- Commission research to understand nuances of communication around their specific treatments/conditions and use the findings to create materials to support effective conversations. These may include unbranded quizzes and information to provide patients with effective language to describe symptoms, “how to talk to your doctor” materials and key communication points for HCPs that include common patient language and clear terminology to use in discussions.
Insights agencies
- Incorporate CHC principles into market research projects with a focus on understanding the HCP-patient dialogue.
- Understand emotional barriers and drivers associated with uncomfortable or embarrassing conversation topics and provide effective tips for initiating those discussions and maintaining their intended flow.
- Recognize and retrieve patient-friendly language (mirroring words, themes, values, analogies) from research for providers; include a lexicon.
- Build tip sheets for talking to patients and “how to talk to your HCP” resources (such as, “10 topics to discuss with your HCP during your next visit”).
References
1 Donnelly, T., et al. “An incomplete diagnosis: Low health literacy and its impact on marketing research.” Quirk’s Marketing Research Review. October 2017.
2 Donnelly, T., Barakshina, T., Kirk, J., Stone, B., and Ashley-Collins, H. “Clearly better: Study underlines the importance of clarity in doctor-patient communication.” Quirk’s Marketing Research Review. October 2020.
3 Donnelly, T., Haimowitz, B., Barakshina, T., Sahni, K., and Russell, H. “The heart of the matter: Communicating with limited-English-proficiency patients in the U.S. emergency rooms.” Quirk’s Marketing Research Review. May/June 2025.
4 Song J., et al. “Detecting language associated with home healthcare patient's risk for hospitalization and emergency department visit.” Nursing Research. 2022 July-August 01;71(4):285-294.