Empowering or powerless?
Editor's note: Tom Donnelly is vice president, head of medtech, at research firm Branding Science. Dave Norton is founder and principal of research firm Stone Mantel. Mary Putman is lead digital strategist at Stone Mantel. Christophe Carington is senior research executive at Branding Science.
Do patients find your health care technology stupid, dumb, smart or genius? Stupid technology uses data incorrectly, making the experience unnecessarily difficult. Smart technology uses data to make health care experiences easier or better than they used to be. As technology progresses, so do patients’ expectations. As more offerings enter the market, digital health tools must go beyond simply “doing the job” and support empowered patients. This is the idea behind genius technology – turning what was a medical condition into a superpower. Is your current digital health care solution stupid? How could you update it to be smart or genius?
Answering questions such as these is part of the work of the Digital Healthcare Collaborative (DHC), a collection of thought leaders from pharmaceutical manufacturers, solutions providers, medical systems and health insurance companies providing thought leadership, collaboration and consumer research as part of an innovation process. We focus on the future of patient/population experiences and engagement, solving for the next two to five years. The real strength of the group is that we are trying to tackle a common problem and are not limited to the lens of one company.
In this article we will provide more background on the work and purpose of the Digital Healthcare Collaborative; describe the research methodologies we use; and illustrate two frameworks that guided our recent work.
Then we will present findings on questions posed by the DHC:
- How is technology currently playing a role in peoples’ health care? What are their needs when it comes to health care? And do they feel comfortable sharing the data required to fulfil their needs?
- When it comes to individualizing and predicting aspects of genius tools in health care, which aspects are most important to patients?
- How can we use technology to improve the patient journey experience?
Year-long program
Each DHC engagement is a year-long program following an academic year. Here is a snapshot of the program in 2019-2020:
The group wrote a charter that everyone agreed was the main mission for the year (summer 2019). There was a secondary research review and an initial round of ethnography to get information on the topic from specific patient types. We met in-person (September 2019) to review the preliminary research and create initial strategic frameworks. Then we had another round of qualitative research (October 2019). Next, we had our second in-person meeting (November 2019) to discuss the research findings and develop company-specific experiences. We learned about these health care experiences in two rounds of co-creation sessions with the different patient groups (December 2019-January 2020). We met again (February 2020) to review the research and finalize each company’s concept to test in a large quantitative survey (March-April 2020) with over 1,000 people. Finally, we had virtual meetings (May 2020) where the findings were shared and discussed.
While the collaborative members gained a substantial amount of insight throughout the year-long engagement, in this article we are focusing on high-level insights from the quantitative study.
Our main focus will be on the key results of a 20-minute online survey of over 1,000 patients conducted in March-April, 2020. The respondents were adult smartphone users and had to fit one of the following criteria: had an acute medical event in the past year (involving surgery/hospital stay or an urgent, emergency medical event); diagnosed with a chronic condition; currently focused on/interested in improving their health and wellness.
In addition, respondents had to meet the needs of at least one DHC member’s criteria to provide feedback on at least one of the member’s concepts.
The data presented here are for n=1,064 demographically representative sample of the United States population provided by Dynata from its sample panel.
Now we will describe two frameworks used in this study: stupid, smart and genius solutions and health care superpowers.

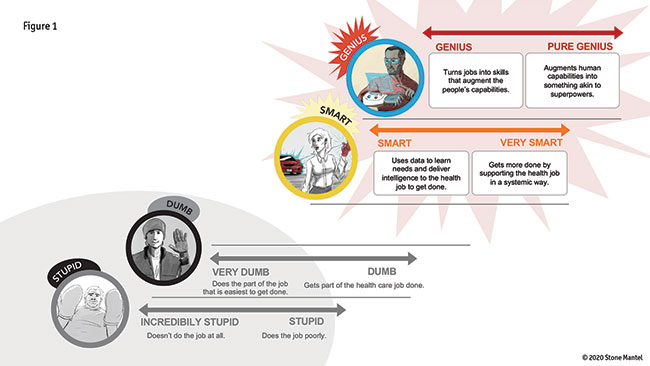
As shown in Figure 1, we developed a framework around solutions to consider what consumers will want and where current solutions stand. They fall into four main categories: stupid, dumb, smart and genius. We will refer to jobs, a framework Clayton M. Christensen developed around the “jobs to be done”¹ concept. Instead of focusing on your product’s features, he suggested focusing on things people want to accomplish, aka a job to be done.
A stupid solution uses digital information in a way that makes the task difficult or misuses the data or is expected to use data and does not. A stupid digital solution gets in the way of accomplishing a job. It does the job poorly. An incredibly stupid solution does not do the job at all.
A dumb solution has no data and therefore does not use digital information to help it get the job done. The solution (which is not digital) gets a limited set of jobs done. In health care, a dumb solution can only get part of the job done. A very dumb solution only does the part of the job that is the easiest to get done.
A smart solution uses digital information to go beyond the original set of jobs to accomplish other jobs and/or adapts to the individual. It uses data to learn needs and deliver intelligence to the health job to be done. A very smart solution gets more done by supporting the health job in a systemic way.
A genius solution turns the job into a skill and augments the user’s capabilities to meaningfully improve their health outcomes. A pure-genius solution augments human capabilities into something akin to superpowers.
Change the way they think
As we applied this framework to health care, we learned throughout the year-long research program that smart solutions change the way consumers think about health care. While historically consumers were willing to accept health care services that did “part of the job,” our qualitative research revealed that consumers want services that do the whole job or the job in a systemic way. Here are examples of each type of solution:
Stupid: Even though your health history is saved on your doctor’s system (has data), every time you visit you must spend 10 minutes answering the same questions about your health history and the system does not use it.
Dumb: You have an inhaler that helps during asthma attacks (gets the job done) but has no data to track your usage over time. Note that non-digital solutions, such as a paper patient chart, can also be called dumb in the context of digital; however, the non-digital solution may work well, especially in comparison to a stupid solution.
Smart: You use a smart inhaler that also syncs with an app to track use. Your doctor can then provide feedback on inhaler technique based on this data (makes the experience better).
Genius: Your data from a smart inhaler is linked with your health record, GPS and weather patterns. The app then alerts you of potential asthma triggers as you’ve had health issues in similar weather previously (job turns into a skill that meaningfully improves health).
Difficult to imagine
Unlike consumer technologies, we discovered in our qualitative research that is it difficult for people to imagine genius health care let alone discuss it. Health care superpowers recontextualize technology in a more intuitive way, allowing patients to describe what their health care needs are and what pure genius looks like in health care. The superpowers were developed from earlier qualitative work done with patients around the topic of stupid, dumb, smart and genius solutions.
- Health foresight: My doctors and my tools work together with me to foresee preventable health issues I am prone to and help me stop them before they start. They also help me understand factors that affect my risks and my symptoms.
- Lifestyle configuration: I know exactly what to eat, how much to eat, how much sleep I should get, how much water I should drink and what exercises work best for me and my health.
- Mind-shifting: I can flip a switch in my mind and suddenly I’m in a different mode. I can go from stressed to relaxed at any time. My willpower is strong when I want it to be.
- Body intuition: Just like a car diagnostic tool but for my health, I can identify information ranging from when I need to go in for maintenance or why my “check engine” light just came on.
- Hyper-understanding: I completely understand my diagnosis, treatment plan, symptoms, medication and options. I feel heard and understood when communicating with health care professionals.
- Information-sharing: My health history can be communicated instantaneously to all my doctors – it’s like they have the same brain!
- Memory champion: I know when my medications were taken and when they should be taken. I clearly remember and convey my health history. I also know when to go in for health checkups.
- Just-right motivation: I am alerted to specific activities that match my interests and location and genuinely help me stay motivated.
Results
Now we will describe findings on the first set of questions: How is technology currently playing a role in people’s health care? What are their needs? And do they feel comfortable sharing the data necessary?
Current digital use of health care information
We found that two-thirds of our sample use digital health tools to manage their health care, which is not surprising given that respondents were required to own a smartphone. Top health care activities on their smartphone include: read about their condition or treatment (40%); track/monitor fitness activities in an app (35%); research latest developments about a condition (30%); track/monitor health in an app (25%); watch videos about their condition (21%); visit a pharma company website (16%); and read/participate in discussions in communities or chat rooms on social media (15%).
We have been tracking digital health care activities. Overall use is slightly up this year from 59% to 66%, though the engagement of specific types of activities varies.
Unmet needs in digital health care
We gave respondents definitions of stupid, smart and genius solutions and asked what percent of their current digital tools fit into each. Among the two-thirds who use digital health tools, one-fourth of tools are considered stupid, half are considered smart and one-fourth are considered genius. We were surprised that these respondents considered as many as a fourth of their digital health care tools to be genius solutions. This may have been more aspirational than actual because the vast majority of health tools today are not in this category yet. Still, it does show that people are eager for genius health care tools.
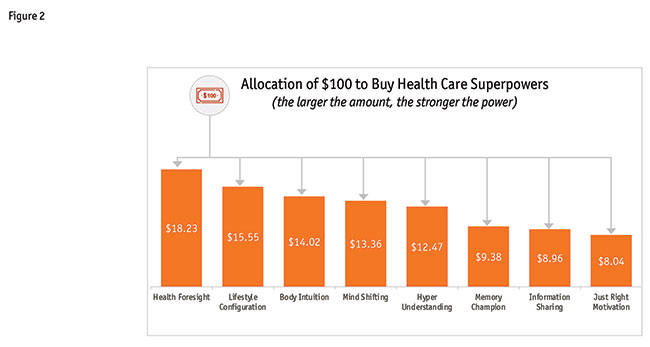
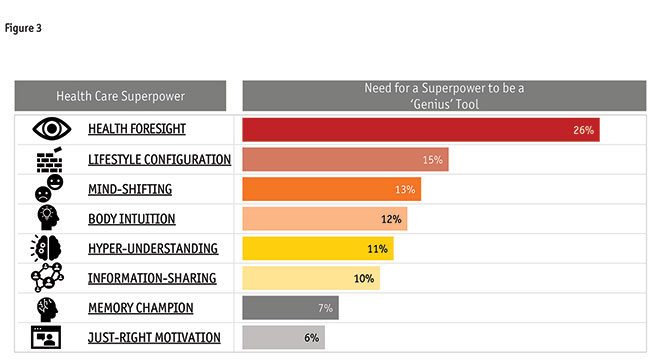
We asked respondents to allocate $100 across the health care superpowers developed in the qualitative research. As you can see in Figure 2, all superpowers were considered to have some value. However, when we restricted people to only picking a single tool, prediction (health foresight) was selected by one-fourth and individualization (lifestyle configuration) was a distant second (Figure 3). What health care superpower would you pick?
Most important aspects of genius technology
Digging deeper to the No. 1 desired health care superpower, we asked respondents what they most desired from a prediction-oriented tool. The benefits centered on early identification of medical issues, including: using information about myself to predict issues such as disease progression and side effects (34%); predicting flare-ups (14%); anticipating stress (13%); forecasting genetic predisposition to certain conditions (11%); using information from people like me to predict issues (9%); and predicting health based on my behaviors (8%).
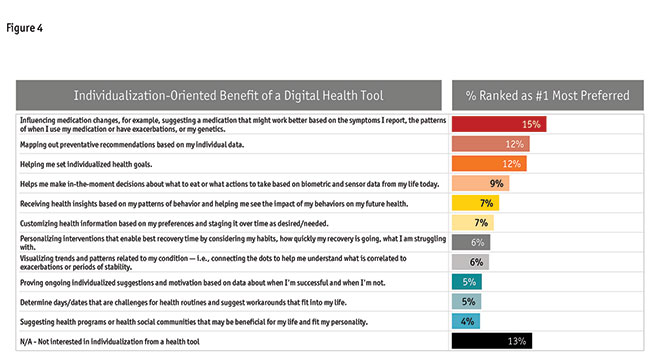
Examining the No. 2 desired health care superpower, we asked respondents what they most desired from an individualization-oriented tool (Figure 4). The benefits centered on preventative recommendations, reinforcing the desire to predict and avoid health issues. This included: influencing medication changes; mapping out preventative recommendations; and helping with in-the-moment decisions.
Given that data is needed to fuel a genius tool, we will discuss patients’ comfort in sharing their health care Information.
Comfort in sharing data
Since 2015, we have been studying consumers’ willingness to share data and with whom they are willing to share it. In 2020, we found that three-fourths of our respondents were comfortable sharing at least one type of data if it would make a digital tool genius. The main reasons they would share their data are: predicting issues (36%); help tailor health programs (33%); and benefits provided toward health goals (28%).
The data types respondents would share include more traditional health data, such as clinical data from home health monitoring data and medical records/history. Fewer people were willing to share non-traditional data such as emotional data, genetic data and GPS location. As you might expect, patients are much more willing to share their health care data with their doctor compared to an insurance company.
Given the need for data to be shared for a smart or genius tool, we created a scale called Context Comfortable based on how comfortable people are in sharing their data and with whom they were willing to share it. Using our scale, we can segment people into four groups: High Comforts, Comforts, Reluctants and No Comforts.
No Comforts (12%): They avoid sharing personal activities or information with digital health care tools in any way and at any frequency. They use digital tools on a limited basis and view any attempts to personalize experiences as invasive. In many cases they are unaware of the level of sharing that is occurring already and fail to link the value they get with data sharing.
Reluctants (39%): They need to understand the benefits they will receive and are willing to share data in specific situations that benefit them. Comparable in their ownership of electronic devices as Comforts. Their attitude toward smart technology in general is less embracive than in the other higher-comfort segments. However, there are some who are receptive to what future technology offers.
Comforts (37%): They also have a fair number of electronic devices and some do use devices that track and report biometric data. The majority are receptive to anticipatory technology from a health care aspect but less so from other aspects. They frequently use digital on a daily basis to help achieve their goals though they do not use as many avenues as High Comforts. Comforts are open to smart experiences and would like their data to be used to improve their experiences but they are less frustrated when it is not used.
High Comforts (12%): They have markedly higher levels of comfort with digital health care tools and the impact of all things digital on their lives. They see value in connecting with a health care tool through digital and expect value in return. They expect digital to facilitate and streamline information flow, providing users with content they want as a result of their health care tool connection and are frustrated when their data is not used to improve experiences.
We constructed the scale based on willingness to share a variety of data, such as wearable data, mobile app data, medical history and clinical data. We also looked at who people are willing to share it with, such as their doctor, family/friends, medical insurance, other app users, their employer, the government and a pharmacy. Often, designers are concerned about the Reluctants and No Comforts groups but typically we are not designing a smart or genius solution for those groups. Early in our use of this scale, there was movement year over year toward people becoming more comfortable but the last couple of years have been stable.
Technology improving the patient experience
Our sample included three types of patients: those who experienced an acute event; those who have a chronic disease; and people on a wellness journey. We examined their preferences for where in their journey a genius solution would be most desired.
Acute event journey: For the acute patients, they would hope for a genius tool to help with the onset of an acute event. They expect that a wearable tool would be an important input of data to allow such a tool to be genius. Other data sources they feel would help include: their medical record; medications and supplements; and their personal goals.
Chronic patient journey: Chronic patients also look at the beginning milestone of the chronic journey as the ideal place for a genius tool to help with initial signs and diagnoses. They would also look for help in controlling their condition. Some of the data they expect would help includes: home health device; emotional health; personal goals; and their medical record.
Wellness journey: Wellness respondents also feel that getting help at the beginning of their journey would be most helpful. They would look for help with: individualized planning; initial motivation; when struggling; and at wellness visits. They expect data needed will include: wearable data, emotional data, personal goals and their medical records.
Conclusions
To summarize, we will review the key questions and our findings for them.
How is technology currently playing a role in people’s health care? What are their needs when it comes to health care? And do they feel comfortable sharing the data required to fulfill their needs? Technology plays a role in consumers’ health care, with their largest unmet needs being the ability to predict health issues and individualized recommendations to manage their health. At a high level, consumers are willing to share data but they may not initially feel comfortable sharing the data needed. Solution providers need to be clear on the value of sharing this data.
When it comes to individualizing and predicting aspects of genius tools in health care, which aspects are most important to patients? Prediction of preventable health issues and understanding the steps necessary to avoid them combine to form consumers’ No. 1 unmet need. Individualization needs of consumers are more varied, though a top need is the ability to map out preventative recommendations – reinforcing consumers’ desire to predict and avoid health issues.
How can we use technology to improve the patient journey experience? People feel that data can be used to improve different milestones within different patient/wellness journeys. The common thread among all types of journey is the need for a truly helpful health tool during the initial milestone of their journey.
Creating meaningful experiences
So, what is the current focus of the collaboratives? We focus on the near-term future of experiences and engagement. We will help you discover and uncover new, universal principles for delivering meaningful health care experiences. This year’s challenge is creating meaningful experiences for now and going forward including digital and virtual delivery. We are providing more linkage between the consumer and health care collaboratives. We have four tracks and members can follow as many of the tracks as they wish: meaningful motivation; meaningful technology; new family dynamics; and health and well-being.

Figure 5 shows the planned schedule for 2020-2021. You can see for each season the research we will conduct, the deliverables we will provide and the outcomes we anticipate. While we seat new members at any point across the year, those involved earlier will shape the year-long plans.
We would like to invite you to consider joining the collaboratives! Why?
Thought leadership: We interact with experienced strategy and design experts. We challenge your assumptions. We share new paradigms.
Collaboration: You accomplish more through collaboration. You work with talented people in other companies. We use innovation processes.
Consumer research: We gain insights from a large consumer sample and do deep insight and co-creation work to help you shape your ideas. If you are interested, please contact us!