
Clearly better
Editor's note: Tom Donnelly is vice president, head of medtech at Branding Science, Doylestown, Pa. Tatiana Barakshina is founding partner of Bazis, Naperville, Ill. Jim Kirk, now retired, is former vice president of Quintiles, Weymouth, Mass. Bill Stone is director, content strategy at Sommer Consulting, Langhorne, Pa. Heather Ashley-Collins is vice president, research solutions at Schlesinger Group, Baltimore.
 Health literacy (HL) is normally thought of as a patient skill that allows them to understand important written information about their health care. In fact, HL spans both written and spoken words and effective health care communication requires that it be used not only by health care users (i.e., patients) but by health care professionals as well.
Health literacy (HL) is normally thought of as a patient skill that allows them to understand important written information about their health care. In fact, HL spans both written and spoken words and effective health care communication requires that it be used not only by health care users (i.e., patients) but by health care professionals as well.
In this article, we: provide context for a current research study on physician-patient communication; describe the method of our qualitative research with both cohorts; discuss the key findings we learned about physician communication styles; and present implications for researchers, providers and marketing communication (marcom) professionals.
Background
The Intellus Health Literacy Initiative (HLI) is a coalition of volunteers dedicated to harnessing the power of health literacy in market research to improve patient outcomes. The HLI was established in 2014. Since that time, we have created original content, conducted novel research and spoken at national conferences to increase awareness of the vital role that health literacy can, does and should play in the health care market research industry. The research study discussed in this article is an extension of a survey we administered to patients, physicians and pharmacists. The results of the study, reported in an article in the October 2017 issue of Quirk’s,1 validated that optimizing written materials (such as booklets, patient package inserts, flyers, newsletters, etc.) with HL best practices improves comprehension for individuals at all levels of HL.
While optimizing written materials is important, physicians’ counseling styles play a pivotal role in patient outcomes. The objective of the current research project is to better understand how the communication styles of health care providers (HCPs) vary based on how they categorize patients’ ability to process important health care information. Our research showed the interconnectedness of written materials and the physicians’ fundamental approach to counseling.
Methodology
As shown in Figure 1, in Phase 1 of this project, hypertension patients with limited (LHL) and adequate health literacy (AHL) discussed their respective health journeys and reacted to a patient decision guide. In Phase 2, patient vignette video clips that were created from the Phase 1 patient research were shown to HCPs to provide context for the HCPs to role-play their counseling interaction with patients. We asked the physicians to summarize how they use currently available written materials to support their counseling and how they would or would not use materials built on the principles of HL.
Figure 1
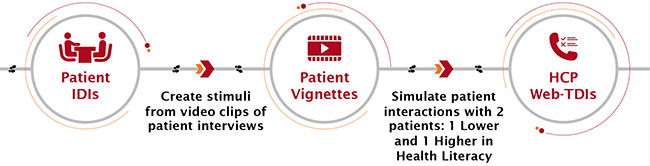
Patient IDIs. Ten diagnosed hypertensive patients who started on a prescription for high blood pressure within the past 12 months were recruited by Schlesinger Group for 60-minute in-person in-depth interviews (IDIs). Their health literacy levels were initially assessed during the screening process using what is commonly referred to as the forms question: “How confident are you filling out medical forms by yourself?” Research reveals that this metric has a .74 to .84 AUROC (area under the receiver operating characteristic) (p<0.05) with health literacy levels.2 We used this question to swiftly assess health literacy levels of potential study subjects, aiming for sufficient representation of both limited and adequate health literacy respondents in the research. Participants’ health literacy levels were ultimately validated using the newest vital sign (NVS), administered when they arrived for the interviews. They were segmented into one of two groups: those who were likely to have lower health literacy and those who were likely to have adequate health literacy.
The interviews were videotaped and they included a guided discussion about the participants’ hypertension diagnoses and their reaction to a printed patient handout on hypertension. The handout was intentionally designed to be non-health-literacy optimized (e.g., it included complex words instead of plain language terms such as “exacerbates” instead of “worsens,” “renal failure” instead of “kidney problems” and “sodium intake” instead of “salt levels”). This encouraged questions from the patients and it provided opportunities for physician counseling and commentary on the handout. Team members who could not be in-person watched via FocusVision.
Patient vignettes. Videotaped interviews with four of the 10 patients were selected to create five-minute vignettes. Two vignette pairs featuring one patient with higher health literacy and one with lower health literacy were created. The pairs represented patients of the same gender and race (two white males and two black females) to eliminate gender and race as variables contributing to any observed differences in physician communication. These video clips were used as stimuli in the physician research.
HCP web-TDIs. Twenty HCPs who treat hypertension (15 PCPs and five cardiologists) were recruited by Schlesinger Group to participate in one-on-one, 60-minute, web-enhanced tele-depth interviews (web-TDIs). Civicom provided its web-platform, technical support and facilitation, helping to get HCPs logged on. After discussing HCPs’ typical approach to hypertension patient interaction, HCPs were then engaged in a role-playing exercise in which they counseled two patients – one with higher health literacy and one with lower health literacy – using the patient vignettes. Order of higher vs. lower HL vignettes was shuffled across interviews, with vignette pairs (white males and black females) also varied across HCP interviews.
Results
We analyzed our findings, using Excel-style transcripts by SyncScripts, to address three major questions:
- How do HCPs group their patients and is health literacy considered?
- How does HCP communication vary by the HCP’s perception of the patient’s health literacy?
- How do/would HCPs use patient education materials?
How do HCPs group their patients and is health literacy considered?
HCPs use different cues to group their patients: ability to articulate their questions and concerns; motivation or likelihood of compliance; capacity to correctly “teach back” what the physician just communicated to them; level of education and profession; having a medical background; and clothing.
While most physicians buy into the concept of HL, the term was not universally used. Some physicians volunteered terms such as “comprehension” or “understanding” in discussing HL but then went on to say that these terms are more the result of HL rather than a synonym for it. Despite the general agreement that HL is important to consider, as many as one-third of HCP respondents misidentified patients’ level of HL.
How does HCP communication vary by the HCP’s perception of the patient’s health literacy?
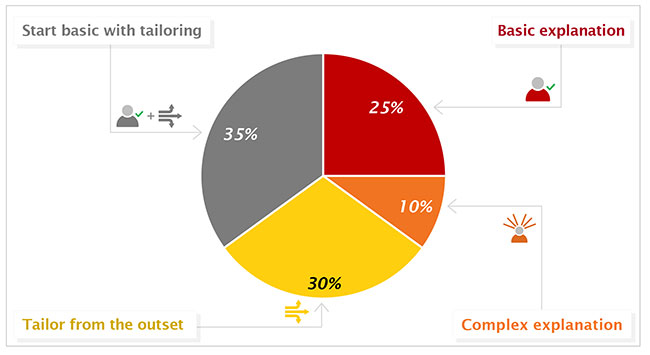
Many HCPs tailor counseling based on their perception of their patients’ understanding. This tailoring includes the content of the HCPs’ verbal interaction, how quickly they move from one topic to another and the structure and complexity of their spoken sentences. Four strategies for counseling emerged (Figure 2):
- Everyone receives a basic explanation (25%) – physicians rely on patients’ unsolicited questions and self-guided web searching to supplement their understanding.
- Everyone receives a more complex explanation (10%) – these physicians feel that they should put forth a full explanation to every patient.
- Physicians tailor the content and language from the outset (30%) – these HCPs rely on their assessment of the patient’s literacy and comprehension level from the beginning of interacting with the patient (some say they rely on their nurses to give them a heads-up on how ready the patient is to hear their message).
- Start with a basic explanation with tailoring after initial reactions (35%) – this was the most popular approach and was claimed by the physicians as the most responsive and responsible.
Figure 2
Some physicians try not to assume a particular level of HL. Their initial counseling of patients generally assumes a basic level of understanding, which they check throughout their interactions. While most physicians noted the patients’ reaction to our handout, they did not base their counseling strategy on that reaction.
How do/would HCPs use patient education materials?
There was a surprising lack of consistency and an absence of specific organization of patient education materials. Typically, physicians use materials that are more conveniently accessed, with little attention dedicated to the format and language of the materials. A few use canned materials (e.g., AAFP, AHA), particularly if they are available as standard printouts from their electronic health records system. Two physicians mentioned that the EPIC system has a particularly useful handout. Some HCPs use a handout on the DASH diet as a useful starting point for discussion about diet and lifestyle. A few physicians say they create their own handouts to summarize the condition and its management. Regardless of their approach to written materials, most rely on verbal explanations as the most flexible and useful way to interact with patients because they can readily tailor explanations to individual patients. The handouts used are often for patients to take home rather than used during the discussion.
Most HCPs and patients picked up on several elements (noted earlier) in our handout that were purposefully not optimized. This shows that physicians and patients can identify the difference between a more complex and a health literacy-optimized handout. Despite this ability, HCPs do not focus on providing patient education material that can be easily understood by all.
When asked how interested they would be in a modified handout or multiple handouts, most HCP respondents said they prefer one version that is basic and understandable by all. Although a few suggested having an additional, more detailed version for higher-comprehension patients, most physicians were concerned about the time needed to manage multiple versions. Regardless of what is provided, most would continue to rely on verbal interaction with patients, either in place of written materials or as the core of a package of counseling.
Discussion
The objective of our HL initiative is not simply to improve written materials but rather to enhance the overall quality of health care communication, to empower patients in managing their health and to encourage health literacy best practices among physicians. One of the overwhelming impressions from the HCP interviews is that the physicians are generally interested in maximizing the effectiveness of their counseling. All HCPs are limited by the time demands of modern health care practices and some see written materials as a valuable resource for supporting counseling.
Our research shows that doctors should start conversations in plain language with all patients because:
- Physicians are inaccurate judges of patient health literacy.
- Patients at all health literacy levels will understand their disease and treatment better.
- Patients with higher health literacy will have a chance to ask more questions and connect with their doctors.
Figure 3
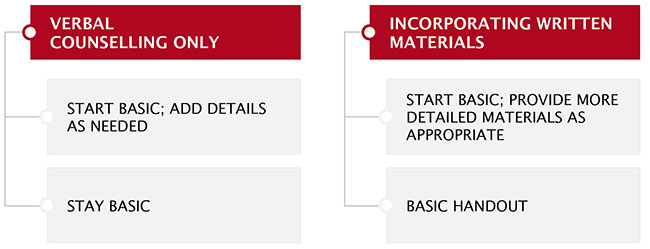
This recommendation holds up whether written materials are involved or not. This approach can be used in four basic counseling strategies depending on whether written materials are used and whether physicians provide more detailed information to select patients (Figure 3).
This research showed that counseling is itself dependent on patients’ ability to comprehend and act on critical health information. Physician training should provide greater focus on health literacy and comprehension. The approach of starting basic, regardless of the availability of health literacy optimized materials (paper or web-based), will ensure that the largest proportion of patients will be effectively served.
Implications
Patients come from a variety of backgrounds and their level of HL inevitably varies. In a time-constrained environment of direct interaction, it is impossible for providers to accurately judge the HL level of all patients. Our findings led to important implications for insights professionals (including industry market researchers and clinical researchers), health care providers across specialties and marketing communication specialists – anyone contributing to the development of patient decision aids and written information embedded into EHR systems.
Researchers
Researchers should take HL into account in four areas: recruitment, participation, stimuli and analysis.
Recruitment. Lower-HL respondents engage in market research at a lower rate compared to those with higher HL. In addition, the industry tends to systematically remove lower-HL respondents from market research because we screen out those who are vulnerable to being lower in HL (e.g., lower SEC, older populations, minorities, on Medicaid, less articulate, less able to engage in interviews). When developing information for patients and excluding those with lower HL, the outcome will ultimately fall short to the detriment of both lower and higher HL patients.1 Researchers should use special recruitment techniques, such as pre-recruiting with the forms question and confirming HL level with the NVS.
Participation. Providing simple communication of study goals and processes help with respondent comprehension and engagement in the study. When possible, provide both written and verbal instructions. For written directions, using pictures or infographics can help convey meaning. Including an example of the exercise can also give respondents a better idea of what the researcher needs. The actual approach will depend on the study and researchers must be careful not to bias responses by providing the answers sought.
Stimuli. The research stimuli are typically the focus of feedback, such as patient education materials, written instructions for use or a consumer ad. Sometimes stimuli are used for other exercises (e.g., projective techniques, patient journey). Regardless, researchers should follow HL principles3 in designing research stimuli, including vocabulary and language use, font size and style, grouping/chunking, content/scope, use of white space, justification and use of graphics.
Analysis. Separate analysis of lower-HL patients is advised to ensure appropriate and useful insights are uncovered. Regardless of whether it is qualitative or quantitative data, important trends may wash out or be treated as outliers when lower-HL data is not examined separately.
Providers
Health care providers need to ensure that each health literacy group receives an explanation that optimizes patient engagement and treatment compliance. Our research shows that using a basic explanation as a starting point in both written and verbal communication will optimize comprehension and engagement across all HL levels of patients. Providers should then be prepared to move up to a more tailored explanation if a patient is interested in one. With this approach, patients at all health literacy levels will have a firm foundation for understanding the disease and treatment. Patients with higher HL will get an opportunity to build on their knowledge and involvement, prompting more tailored, detailed communication from providers. Given that providers’ time is limited and that their judgement of patients’ HL is not fully accurate, starting with a basic approach is the best strategy.
Marketing communication professionals
Marketing communication professionals should consider our advice to both researchers and providers. Information conveyed to patients should follow HL principles regardless of the format (e.g., patient education materials, decision aids, consumer ads, etc.). Our research shows that patients of varying health literacy levels all benefit from a simple, basic HL approach (e.g., language at a sixth-grade level, good use of white space and graphical elements, etc.). Thus, marcom teams should consider a tailored, more detailed format of written materials to be available as an add-on to, not as a replacement of, the simple basic approach. Do not rely on physicians to correctly identify which of their patients should get a simple versus a more detailed handout because they often incorrectly identify HL levels. Motivating patients to act starts with them understanding.
Broad array of styles
We found that HCPs use a broad array of styles for counseling patients and that a range of market research techniques is needed to uncover these dynamics. While this research was focused on HCPs’ communications with patients, other dynamics include patients’ interactions with others across their networks (such as other HCPs, other medical staff, family, friends, colleagues) and various sources of information beyond what their doctor provides (whether via the Internet, TV, radio, magazines, newspapers, books, etc.). In this study, we demonstrated that health literacy affects such fundamental issues as patient comprehension and confidence, as well as physicians’ sense of job satisfaction and efficient use of precious time. Both the transmission of information and the instilling of motivation depends on how well patients, HCPs and the health care system connect. Researchers, providers and marcom teams should take health literacy into account so that they can better help patients live healthier lives.
Intellus’ HLI will continue to educate the community, as well as conduct research, including an experimental study to examine the relationship between literacy demands and patient behavior. (We are proud to announce that we won the Institute for Healthcare Advancement Health Literacy Award in the research category for this study!) If you are interested in joining our group, partnering on future studies or would like our consultation in health literacy, please contact us!
References
1 Intellus (formerly PMRG) Health Literacy Initiative Committee: “An incomplete diagnosis – low health literacy and its impact on marketing research,” Quirk’s (October 2017).
2 Chew, et al.: “Validation of screening questions for limited health literacy in a large VA outpatient population,” Journal of General Internal Medicine 23.5 (2008): 561-66.
3 Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. (2013). CDC Clear communication index: a tool for developing and assessing CDC public communication products: user guide. http://www.cdc.gov/ccindex/