
Zebras do exist
Editor's note: Wes Michael is president and founder of Rare Patient Voice, a Towson, Md., research firm.
 In the rare-disease community, you hear a lot about zebras. Why? In medical school, students are taught, if you hear hoofbeats, think horses, not zebras. That makes logical sense. What is the most likely diagnosis? It is more likely to be a common “horse” than a rare “zebra.” But, as you hear over and over from rare patients, zebras do exist. And physicians need to be aware of when to go beyond the horse to spot the zebra. Because the longer they suspect a horse, when it really is a zebra, the longer it will take to get to the correct diagnosis. And that means a longer time without treatment.
In the rare-disease community, you hear a lot about zebras. Why? In medical school, students are taught, if you hear hoofbeats, think horses, not zebras. That makes logical sense. What is the most likely diagnosis? It is more likely to be a common “horse” than a rare “zebra.” But, as you hear over and over from rare patients, zebras do exist. And physicians need to be aware of when to go beyond the horse to spot the zebra. Because the longer they suspect a horse, when it really is a zebra, the longer it will take to get to the correct diagnosis. And that means a longer time without treatment.
I was recently at a rare-disease conference and a patient said, “We talk a lot about finding out about the patient journey. Please don’t call it a journey. A journey sounds like something you’d find enjoyable. Please call it an odyssey. That is more accurate. It is not a fun experience.”
How true! What is the patient odyssey? How does it vary by disease? We set out to survey our patients and caregivers to find out their perspective. We asked patients or their caregivers about their disease, which (if, as is common, they have more than one) was most difficult to diagnose, and then, for that disease, how long it took to get diagnosed. We also asked how many medical tests they required, how many physicians they needed to see, were they misdiagnosed along the way, if they had genetic testing and if they experienced a delay in treatment. We provided the opportunity to explain in an open-ended fashion their experience.
There are about 7,000 rare diseases. We surveyed 3,471 of our patients and caregivers across 436 different diseases. We’ll focus on totals, several instructive diseases and results from those diseases where there are 10 or more responses. The results may not be representative, as respondents more interested in sharing their negative experiences in the diagnostic odyssey may be over-represented. But you’ll hear the authentic voice of the patient. And we are happy to share freely the data to any interested parties.
A much more extended wait
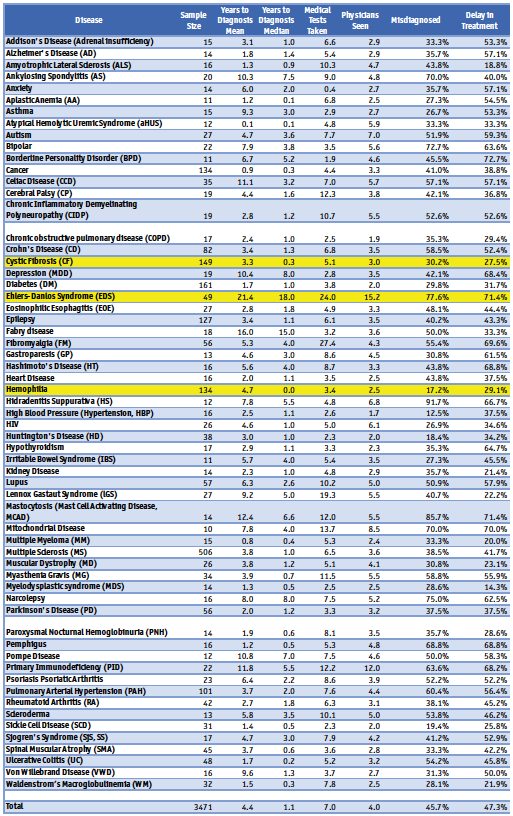
The story of the diagnostic odyssey is more relevant as 436 separate odysseys, as each disease or condition reveal different results. But let’s start with some totals. Across all the conditions, the average (mean) time to diagnosis was 4.4 years. The median time, however, was 1.1 years, indicating that half the sample came to their diagnosis in about a year. But it also shows, many had a much more extended wait.
On average, patients had seven medical tests taken to get to their diagnosis and saw four physicians. Nearly half (46%) were misdiagnosed along the way and nearly half (47%) believed their treatment was delayed.
Nearly one-third (30.5%) reported having genetic tests taken and, among those, two-thirds (66.9%) stated that the genetic test led to the correct diagnosis. Three-quarters (76.8%) said their genetic tests were covered by insurance.
Many different pictures
If we look at the 61 diseases where we had 10+ respondents (Table 1), we see many different pictures. Ankylosing spondylitis, celiac, depression, Ehlers-Danlos syndrome, Fabry, mastocytosis, Pompe, and primary immunodeficiency all had a mean of over 10 years until diagnosis! Realizing that a few people that took decades to be diagnosed can drive the mean, we’ve provided the median as well and you can see most of these had a median of over five years until a correct diagnosis. That is a long time to be suffering from an unknown condition! These conditions also typically required a large number of physicians to be seen and medical tests to be taken. And a majority of most also were misdiagnosed along the way. Some conditions (ankylosing spondylitis, Ehlers-Danlos, hidradenitis suppurativa, mastocytosis and narcolepsy) had over three-quarters of the patients misdiagnosed. Nineteen of these 61 conditions had half or more of the patients misdiagnosed. And 30 of the 61 conditions had half or more suffering from delayed treatment.
Let’s look at several of these conditions that represent different experiences in more detail: hemophilia, cystic fibrosis and Ehlers-Danlos syndrome.
Hemophilia
Hemophilia is a rare genetic bleeding disorder. Internal bleeding can damage joints and organs, and thus can be life-threatening. The most common types, A and B, primarily affect males, but females, who are carriers, can also be affected. Since hemophilia is a fairly well-known orphan disease and due to its genetics, families often anticipate the possibility of their child inheriting the condition. So, it is not surprising that the median time to diagnosis is 0 years, with 71% diagnosed in the first year. Many reported that it wasn’t unexpected as they had a family history. But it can also be caused by a spontaneous mutation, which would not be expected. Several reported diagnoses at the time of circumcision. But others weren’t diagnosed so quickly, as the mean time to diagnosis was reported at 4.7 years. One noted: “[The] pediatrician did not believe there was anything wrong. He felt we (parents) were responsible for the severe bruising.” Several reported similar histories, adding insult to injury.
Females made up over half of those who that weren’t diagnosed for 10 or more years. Since genetically it is expected to occur almost exclusively in males, it isn’t surprising that females weren’t quickly diagnosed. Some reported:
“[I] was told that some women just bleed heavily, have anemia, have extended length periods, bleed heavily after birth, bruise easily, just have joint pains. Outdated thinking and resistance to change in the medical community is why I went so long under-diagnosed and under-treated.”
“No one ever looked at hemophilia because I am female. Once my daughter was diagnosed then I was, also.”
“As a woman, I was only labeled a ‘carrier’ even though my factor level is in the 20s.”
The impact of these missed diagnoses is striking. One male patient reported:
“I visited an emergency room multiple times, but the doctors had no idea that my bleeding could be hemophilia.”
Cystic fibrosis
Cystic fibrosis is a progressive genetic disease that affects the lungs and other systems. It limits the ability to breathe over time. Most newborns are now screened for CF, which explains the short time to diagnosis, a mean of 3.3 years and a median of only .3 years overall. Three-quarters (75.8%) reported having a genetic test, which led to the correct diagnosis in over 90% of the cases.
“For us, nothing [could have led to a faster diagnosis]. The diagnosis was made as part of the newborn blood screening that is mandatory in Illinois. He was diagnosed at 12 days and confirmed a day or two later by a sweat test. We started therapy that week.”
“I found out while pregnant. We were very ‘lucky’ as we were prepared at his birth.”
“The fact that they now test at birth and had just started in 2001 made diagnosis all but immediate. Just need all states to be doing this.”
We can see the impact of newborn screening. If we look at patients born since 2000, the average time to diagnosis was .75 years. But for those born before 2000, they averaged 6.6 years to diagnosis. Before 2000, 47% reported misdiagnosis (often asthma, allergies, bronchitis), while since 2000, only 20% reported misdiagnosis.
Ehlers-Danlos syndrome (EDS)
Ehlers-Danlos syndrome (EDS) is group of disorders that affect connective tissues that support skin, bones, blood vessels and other organs. This can result in a range of outcomes from loose joints to life-threatening complications. Various gene mutations have been association with the condition. It is diagnosed by symptoms and in some cases confirmed with genetic tests.
Of all the diseases in our study with 10 or more responses, EDS showed the longest time to diagnosis, with a mean of over 21 years. Over three-quarters (77.6%) were misdiagnosed. EDS patients/caregivers noted taking a mean of 24 tests and seeing over 15 physicians, among the highest in the study. Over 71% experienced a delay in treatment. About half (49%) had taken genetic tests and for two-thirds of them (66.7%) the genetic tests led to the correct diagnosis.
The stories conveyed by the respondents describe an especially difficult diagnostic odyssey, full of misdiagnoses.
“I was called a ‘clumsy child,’ when I would roll ankles or knees or dislocate fingers. As a teenager, ‘accident-prone’ and then each injury was treated separately. Sprained ankle, torn rotator cuff, dislocated foot, jammed thumbs, etc.”
“A lot of doctors were confused by the laundry list of symptoms, not realizing that is typical. A lot of them interpreted that to mean that I was either exaggerating or had somatoform [psychological] disorder.”
“EDS is rare but if someone had put all of my symptoms down onto one sheet of paper and actually tried to see how they connect I think it would’ve been spotted. Instead our health care is very linear. So many blood tests, X-rays, MRIs, more blood tests – mostly because that’s what insurance told them they had to do.”
Sufferers of this rare disease stressed the importance of raising its awareness among physicians:
“[We need] more awareness by other doctors and PTs. I saw multiple orthopedists for sprains and other injuries who never suggested ‘Hey, this could be EDS.’”
“More teaching of EDS in medical schools, more awareness and understanding of the condition among doctors (this has improved in the last decade), more research into treatment and cure for EDS.”
“My diagnosis came from clinical tests, not blood tests. PCPs should use the Beighton score more often as a test. It’s easy to do and costs no money. I think that it should be a standard test when you have joint issues.”
The delay in diagnosis had severe impacts on patient well-being:
“If I had known 28 years ago to not stress my joints, I wouldn’t be as bad as I am today. And if I had known about the common co-morbid diseases, I would have gotten treatment for those sooner.”
 Let respondents answer
Let respondents answer
The questionnaire was designed not to push respondents into preconceived notions about their diagnostic odyssey. So rather than provide lists to choose from regarding misdiagnosis, delays in treatment and reasons for the length of time it took to obtain diagnosis, we let respondents answer those in open-ended fashion. And did they ever! Two-thirds answered the open-ended questions, with an average of 42 words each. It totaled 9,147 open-ends. I read through them all and it felt like the equivalent of doing a thousand IDIs. Their voices came through loud and clear. And for many, they provided a scathing indictment of the medical establishment.
Key reasons cited for delayed diagnoses included:
Voice of the patient. Most often mentioned was that physicians weren’t listening to the patient.
“They told me [the caregiver] it was impossible that her symptoms were occurring.”
“[Faster diagnosis would have happened if] physicians [were] not making assumptions about my pain and symptoms and listening to what I had to say.”
“I know doctors hate it when you come in and you’ve already diagnosed yourself but at least explore the possibility that this patient has put in time and is educated and knows their child better than the damn doctor.”
“Doctors are only relying on test results and not listening to me as the patient.”
Physician mind-set. Physicians weren’t looking for the disease.
“No one wanted to see a zebra – they preferred to convince themselves and me that they were seeing a horse.”
“I was repeatedly told that I didn’t need to be tested for cancer because I was not, and never had been, a smoker.”
“Doctors always thinking something is so rare no one can have it.”
“They kept saying it was nothing, don’t worry about it; was told it was just my depression and anxiety.”
“Doctor was arrogant and assumed that I had diagnosed myself with scleroderma and he thought I was a fat, well off, non-working woman who had given herself an ‘interesting’ diagnosis.”
“They are doctors and I always thought they were supposed to try to resolve my problems. Most never did and sent me away making me think I’m a hypochondriac.”
Bias. Many patients felt there was bias against them due to their gender, race, weight or age.
“Women tend to get undertreated because doctors only half listen/don’t take symptoms seriously, so I thought many of my symptoms were in my head – so I just didn’t go to the doctor until symptoms were really bad.”
“The medical professions overall need to blame everything on obesity as an easy answer.”
“The times I received the most help was usually when I brought my white male partner. It was like he was more credible than the poor, black girl whining about something no one could see.”
“I was a teenager when symptoms started and they kept blaming it on me being a teenager.”
Insurance. Some believed insurance, or the lack of it, contributed to the lengthy diagnosis path.
“Insurance companies need to back off. A few instances, tests had to be explained and proven ‘needed’ before they would be covered. It is sad that insurance companies have a say in a patient’s care.”
“Insurance allowing her to see the correct specialist. We had to wait for a referral from her doctor to get that specialist which wouldn’t have changed the disease however she would have been on drugs over two years before.”
Location. Proximity to the appropriate facilities or specialists was to blame for some.
“I lived in a small rural town and there wasn’t a doctor there that had experience with Crohn’s disease.”
“[We need] more advanced treatment in rural areas.”
“[We need] a better more equipped medical facility in the smaller city I live by.”
Getting to the correct specialist. For many it took a long time to get to a physician who was able to make the diagnosis.
“My physician and first two neurologists were either unaware of or unfamiliar with the disease.”
“Pediatric neurologists should not be afraid or hesitate to refer patients and their families on to a specialist (such as the epileptologist) in cases such as LGS.”
“It’s important to realize that primary care physicians do not have the knowledge or skill to diagnose or treat specific diseases.”
Medical education. Many mentioned that rare diseases aren’t taught sufficiently in medical school.
“[We need] better information in medical books, currently just two lines in a textbook [about Behcet’s disease].”
“Teaching physicians that there is more beyond the 70% that fit into what they learned in medical school, to look and research options when someone doesn’t fit the norm.”
“I believe time spent in med school covering these rare diseases is less than a day and future doctors are taught to look for the obvious, not the rare...The horse, not the zebra.”
State of medical knowledge. In some cases, the blame was placed on the deficient knowledge of the disease at the time.
“The first two patients discovered to have this syndrome didn’t happen until 2012 so I don’t think we could have been diagnosed properly in 2007.”
“There were no doctors that knew what celiac was in 1992.”
“In the ’80s things were just not like they are now. We didn’t have access to the genetic testing like we do now.”
Delay or denial on the patient’s part. Some patients feel they played a part in the slow diagnosis.
“I didn’t want to do a colonoscopy.”
“I figured I could get over it on my own.”
“It was my failure/procrastination to officially be tested.”
“Chose not to tell anyone for 25 years as I would not get jobs or insurance.”
“My husband hates doctors and is not always completely honest when responding to their questions.”
Words of advice
The respondents provided words of advice for everyone involved in the health care process as well.
Patients
“Make suggestions when you see your primary physician!”
“You know your body. Don’t take no for an answer. Be your own advocate.”
Physicians
“Please, listen to your patients. They know when something is not right with their body.”
Medical education
“More time needs to be spent training physicians on rare diseases.”
Patient advocacy organizations
“Raising awareness among physicians and the general public can help put your disease on the map, making sure physicians and patients consider it may be the cause of their symptoms.”
Apply learnings
Perhaps artificial intelligence diagnostic systems, such as Watson, can also extend the ability of physicians to incorporate all the symptoms and test results and apply learnings from the 7,000 rare diseases to properly diagnose much more rapidly than these patients have experienced. As their comments show, no matter which part of the health care system is involved, there is much work to be done to better consider, incorporate and act on their viewpoints.