Editor's note: Kevin M. Kelly is executive vice president and general manager of HRA – Health Care Research & Analytics. Christina Rife is the firm’s vice president, research strategy.
With the implementation of the Patient Protection and Affordable Care Act of 2010 (PPACA), the concepts of accountable care and value-based health care have become a central focus for health care providers. As the U.S. health care system moves away from long-standing fee-for-service practices and embraces a pay-for-performance approach (value-based health care), so too does the relationship between providers (physicians and nurses as well as hospital and health systems executives) and health care manufacturers – whether pharmaceutical, biotechnology or medical device companies. But what is accountable care and what should manufacturers know in order to compete in the new health care landscape?
The term “accountable care” has adopted multiple meanings over the past several years. In their truest intended form, accountable care organizations (ACOs) were established under PPACA to optimize the Medicare Shared Savings Program in an effort to contain costs generated via Medicare Part A and Part B. As a catchphrase, accountable care has come to represent a new health care dynamic of risk-sharing, value-based health care and overall population health management – at a most fundamental level, holding providers accountable for overall quality of care and for the outcomes of that care. The principles of accountable care are codified by the Centers for Medicare and Medicaid Services (CMS) in what is known as the Triple Aim – improving the individual experience of care; improving the health of populations; and reducing the per capita costs of health care. While introduced by CMS and initially impacting only reimbursement for Medicare claims, the principles of the Triple Aim have been adopted and implemented beyond Medicare or CMS ACOs and are now inherent to risk models employed by so-called “commercial” ACOs as well as to integrated health care as a whole.
Relationships and opportunities
Our firm, HRA, recently completed an extensive study on accountable care, its continued evolution and the impact it is having on the relationship between providers, payers and pharmaceutical, biotechnology and medical device manufacturers. Fundamental to a full understanding of the accountable care landscape are the distinctions between the needs of CMS and commercial ACOs, the relationships and opportunities for partnership between ACOs and the health care industry and the ever-changing and important role of commercial payers in accountable care.
An appreciation of the nuances of each of these components could unlock significant opportunity for health care manufacturers to gain a competitive advantage through better targeting of these important segments. Marketing and sales operations within pharmaceutical, biotechnology and medical device companies must develop a better understanding of ACO structures and unmet needs in order to establish more effective programs, more compelling interactions and a better linkage of product efficacy to the outcomes that matter most to ACOs.
Manage and coordinate
By definition, an ACO is a group of providers of services or suppliers that work together to manage and coordinate care for a defined population. CMS-certified ACOs have been approved by the Centers for Medicare and Medicaid Services to provide this level of care for Medicare fee-for-service beneficiaries. Commercial ACOs are those in which a commercial payer partners with providers (physicians, hospitals, home health care services, etc.) to leverage the same general principles defined by CMS in order to promote better quality, more coordinated care with financial benefits and/or penalties associated with adherence to set guidelines – but for patients covered under commercial health care plans.
On the surface, central differences between CMS and commercial ACOs include the identity of the end payer, the specific quality metrics enacted by each group and the defined levels of risk-sharing that apply across each segment. For the CMS ACO, the risk/reward component centers specifically on the Medicare population – failure to provide positive outcomes from care carry the risk of unreimbursed Medicare expenses on the part of the provider. Commercial ACOs, on the other hand, have the backing of a commercial payer and, given the nuances of the commercial payer world, have far more variation in terms of the quality requirements and related payment thresholds.
HRA’s study reveals that the two main changes expected for the ACO models are increased risk-sharing for CMS ACOs and the vast expansion of commercial ACOs. From a CMS ACO perspective, as comfort with the model requirements increases, so does the ACO’s likelihood to increase risk from the traditional one-sided model (where ACOs are rewarded for adherence to the Triple Aim but they are not penalized for failure to meet quality-of-care goals) to a two-sided model where both risk and reward are shared between the ACO and CMS and passing along the increased risk to pharmaceutical, biotechnology and medical device manufacturers. In fact, 2017 represents a pivotal year for CMS ACOs; by law, the majority of one-sided contracts will expire, forcing these organizations into two-sided risk-sharing with CMS or dissolving the ACO. Among commercial ACOs, the market will see significant expansion as major insurers such as Aetna, Blue Cross, UnitedHealth and Cigna increase their ACO presence and penetration. In addition, risk-sharing contracts between ACOs and pharmaceutical manufacturers – once purely hypothetical – are becoming a reality, with 8 percent of CMS ACOs sharing risk with manufacturers and 4 percent of commercial ACOs doing the same.

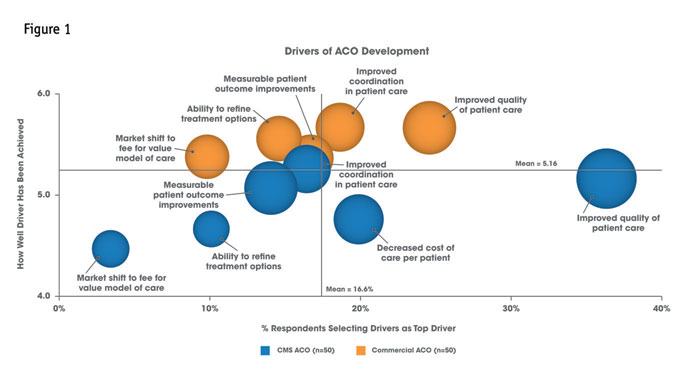
With expansion and change come expanded need-gaps and new opportunities for health care manufacturers to engage with these organizations. The need to improve patient outcomes is a common concern for both ACO types in light of their specific requirements. Further, the challenges of shifting toward value-based reimbursement creates areas of opportunity within both ACO types – although commercial ACOs, grounded and guided by a business direction, are farther along in their evolution CMS ACOs in these areas (see Figure 1). Though specific needs will vary among ACOs, these opportunities may include help with patient access to information, integration and ease of access to computer physician order entry systems (CPOE) or support for discharge programs.
Alters the traditional paradigm
The shift from fee-for-service to value-based health care reimbursement inherent to the ACO model alters the traditional paradigm under which health care manufacturers have operated for decades. As such, manufacturers must adjust their strategies as well as their tactical approaches in order to be in successful partnerships with the ACO customer.
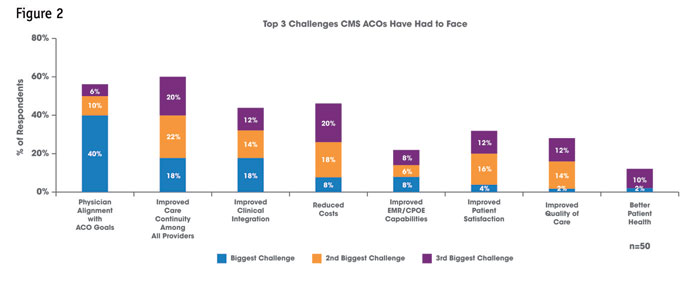
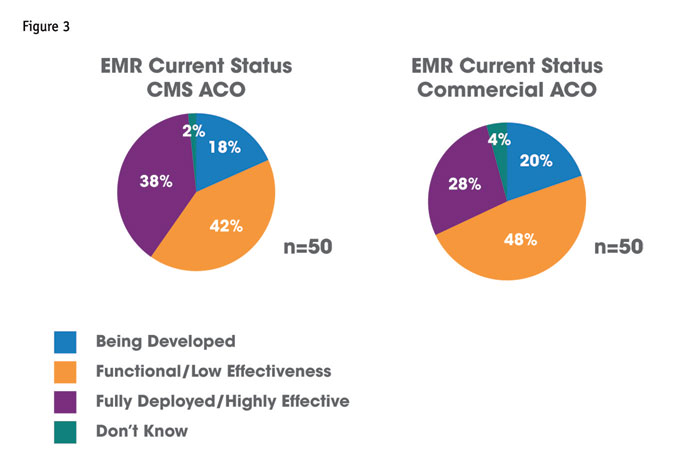
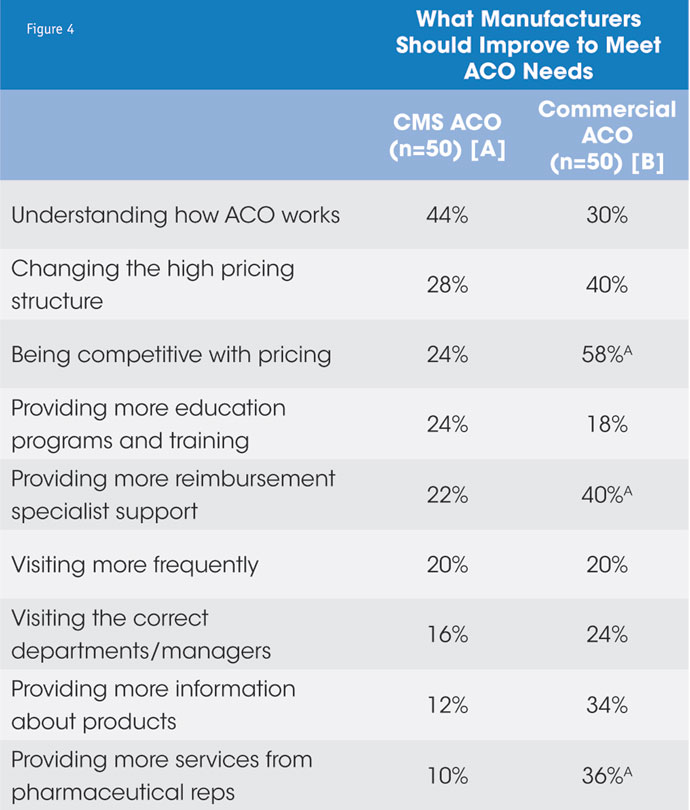
HRA’s research reveals that aligning practitioners under the goals of the ACO remains a key challenge for CMS ACOs, while commercial ACOs seek to improve clinical integration (see Figure 2). As such, the CMS ACO maintains a higher priority for pharmaceutical and other health care manufacturers to understand how the ACO functions and the consequent rules of engagement that exist (see Figure 4). Alignment of the ACO members under an integrated, electronic health records system is paramount to the successful coordination of care that ACOs require – yet neither the CMS ACOs nor the commercial ACOs are satisfied with their progress on this front (see Figure 3).
Philosophically aligned by the overarching need to mitigate financial risk, ACOs seek greater levels of risk-sharing from their manufacturer partners – to see a level of commitment to patient outcomes by having some “skin in the game.” Product benefits can no longer be presented in a silo; their overall value needs to be outlined in the larger context of improving population health and aiding outcomes to meet established quality metrics relevant to the specific ACO. This has become highly relevant with regard to pharmaceutical products used in the management of critical population health concerns, including cardiovascular, metabolic and respiratory diseases. Accountability among patients in managing their own health – especially in the areas mentioned above – also becomes critical to ACO success and the definition of value is intrinsically tied to their ability to contribute to positive patient outcomes by fostering greater adherence and compliance. Commercial ACOs, in particular, seek better pricing, the support of reimbursement specialists and more services from pharmaceutical companies – suggesting that gaps indeed exist and they are looking for help (see Figure 4).
 As ACOs evolve and encounter persistent and new challenges, so must health care manufacturers in responding to these challenges. New, low-hanging opportunities for partnership exist in the form of IT/big data support, patient engagement, risk-sharing and “bigger-picture” value; manufacturers that do it right will prosper in the new health care world.
As ACOs evolve and encounter persistent and new challenges, so must health care manufacturers in responding to these challenges. New, low-hanging opportunities for partnership exist in the form of IT/big data support, patient engagement, risk-sharing and “bigger-picture” value; manufacturers that do it right will prosper in the new health care world.
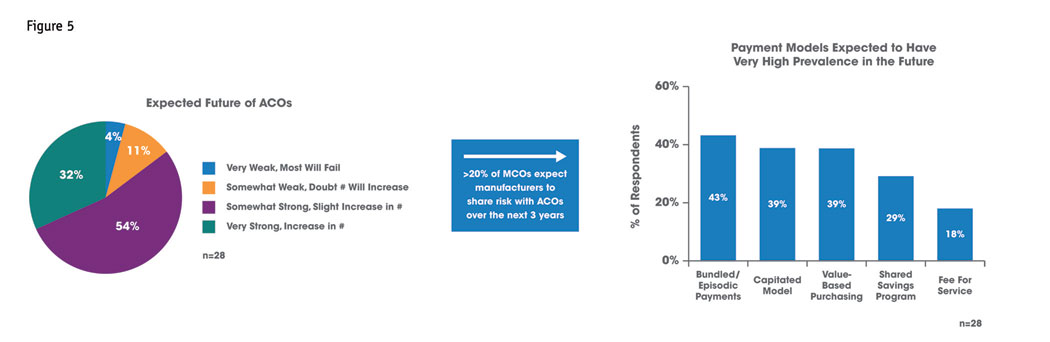
With CMS leading the way toward accountable care, commercial payers were certain to follow. The universal shifting of risk, toward performance-based reimbursement, generates a new role for payers, who largely serve to provide greater structure in this new environment. More than half of payers in HRA’s study are already risk-sharing with ACOs and the expectation is this trend will expand to relationships between health care manufacturers and ACOs. The payer prognosis for the ACO model is strong, with bundled, capitated and value-based reimbursement models becoming the norm (Figure 5). Moving forward, pharmaceutical companies should expect greater pressure from the payer sector to partner more closely with ACOs on addressing adherence/compliance problems, establishing comprehensive discharge programs to limit readmission and assistance in managing high-risk patients.
Cross-functional accountability
Indeed, accountable care is a catchphrase for the new health care dynamic. Success across stakeholders – physicians, payers, patients and health care manufacturers – demands a level of cross-functional accountability unprecedented in the United States health care system. Regardless of the future of the CMS Accountable Care Organization program, value-based health care and the pay-for-performance paradigm is the new reality. For providers, manufacturers and payers, there is no going back – quality is here to stay. The pharmaceutical, bio-tech or medical device manufacturer that can embrace the changing landscape, understand the unique needs of provider stakeholders and institutions, stay ahead of the evolution of the U.S. health care market and be perceived as a true partner by payers and providers alike will have a winning strategy in the end.