Uncovering a hidden partner
Editor's note: Anna Shevalova is healthcare team lead at Bazis Health. She can be reached at shevalova_an@bazisgroup.com. Ekaterina Nemenko is a project manager at Bazis Health. The authors express special thanks to Tatiana Barakshina for her mentorship and also wish to thank Archana Ramakrishna, Bob Spoerl and Vlad Churkin for their contributions to the article.
Our team has spent several years working closely with diverse patient organizations. It has brought us to an understanding useful for the entire health care market research industry: getting to know these communities and learning how to best access them can unlock valuable insights for health care research.
Our article in the November 2020 issue of Quirk’s (“Searching for a common language - Learning from virtual patient communities across the globe”) provided an overview of virtual patient communities and what researchers can learn from them. We decided to build on that research and take it a step further.
First, we tried to explain the difference between various patient communities and conducted a series of in-depth interviews with representatives of patient communities focused on Duchenne muscular dystrophy (DMD) across different countries. DMD is a rare disease that impacts children – primarily young boys – and there is limited medical understanding of it. As a result, it is active with communities of parents seeking answers for their sons on how to help improve their diagnosis.
Our initial hypothesis was that there is a country-specific difference between these DMD communities or at least a difference in terms of stage of development. But the more data we gathered, the better we could see that there is a distinct type of community that we later called “newly formed” that transcends countries and cultural differences. Although the term newly formed refers to a stage of development, our research revealed this type of community is not primarily characterized as young or underdeveloped. Rather, these subsets of patient communities have values that differentiate them from communities we termed “established.”
In this article, we’ll compare patient communities and their value systems and describe newly formed communities as a potential partner for health care market researchers.
The starting point of our analysis was comparing many patient communities we have been working with and those we identified as newly formed. In order to understand what differentiates them and to determine whether there is any community that we as health care researchers should especially consider, we studied Duchenne patient communities across the U.S., India and Russia (Figure 1). We looked at groups that were founded at different times – between 1995 and 2020. Our goal was to compare the modes of organization of the specific communities and their relationships with the international community and pharmaceutical companies. Through this comparison, we wanted to distinguish newly formed communities from established ones.
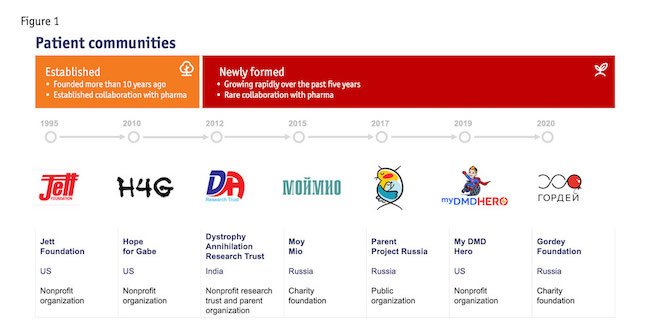 Based on our findings, we classify communities that have been rapidly growing over the last five years and are characterized by rare contacts with pharmaceutical companies and their government as newly formed communities.
Based on our findings, we classify communities that have been rapidly growing over the last five years and are characterized by rare contacts with pharmaceutical companies and their government as newly formed communities.
We categorize communities founded more than 10 years ago and working in close collaboration with pharma companies and government agencies as established.
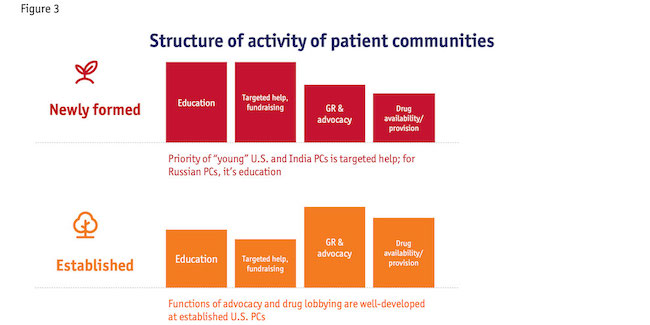
First, we compared the principal focuses of organization in DMD parent communities and discovered newly formed patient communities (hereafter referred to as PCs) are mostly focused on education and targeted help. On the other hand, established communities develop their relationships with governments and pharmaceutical companies. Their tentacles stretch out further in part because of their years in existence and the traction they’ve received because of that. The functions of advocacy and drug lobbying are not developed in newly formed PCs.
Secondly, the comparison of the funding sources of DMD patient communities reveals that newly formed communities are mostly funded through private donations, while established patient communities receive funding from the government and pharma companies. The reason for this is that newly formed PCs tend to avoid direct funding from pharma to maintain their independent status.
We also compared the structure of human resources in DMD patient communities and concluded that newly formed PCs are mostly composed of parents who contribute to the community as volunteers. In short, caregivers with lived experience are principal advocates of patients’ rights in newly formed PCs.
We studied relationships of newly formed PCs with pharma, the medical community and other patient organizations. Our main finding here is that newly formed PCs are rarely connected with pharma and local HCPs but they are open to collaboration with other parent communities within their native countries. They study other parent organizations and prefer to find their own area of responsibility. Since established communities depend more on financial support from pharma and government agencies, they develop independent projects to compete with other communities for funding. This is what differentiates them significantly from newly formed communities that follow a different logic.
Connected in some capacity
As we studied the international relationships of patient communities, we found they are connected in some capacity but at different levels. For example, communities in the U.S. and India are members and even parts of each other’s advisory boards. We found that Russian organizations feel rather excluded from the international community regardless of their personal contacts with some of the international organizations. This is in part due to language barriers some members of Russian groups face. However, we believe that they all are integrated enough to be accessed through international parent organizations.
Finally, we compared the purpose of communication within different parent communities and realized that the members of newly formed communities rarely meet in person; they are mostly online communities that keep in touch through social and messaging platforms such as WhatsApp, Facebook and others.
Based on the data we gathered during the in-depth interviews, we concluded that newly formed patient communities are a recent phenomenon within the last decade. These communities would not be possible without the internet and the nature of how so many people now live. All newly formed PCs are characterized by a particular set of values that differentiate them from established communities and influence their potential value as a partner for health care market research.
Flexibility and relative independence
Let’s now look at the value that newly formed patient communities bring to health care research. As alluded to earlier, this is a particular form of community characterized primarily by its flexibility and relative independence from government and pharma companies. These features often make these communities invisible and tough to access for health care researchers. However, these communities offer a great deal of value to researchers looking for insights.
We argue that in our understanding of patient communities we should focus on their unique value system. Our data shows that one of the principal values for newly formed PCs is online presence. Offline events are rare. Their priority is fundraising and informational support of caregivers. In the case of Russian patient communities, we see they tend to work with the government, as it is the only way to affect change on the national level. But in America and India, new PCs tend to avoid contact with the government. Typically, they do not seek nor expect funding from the government.
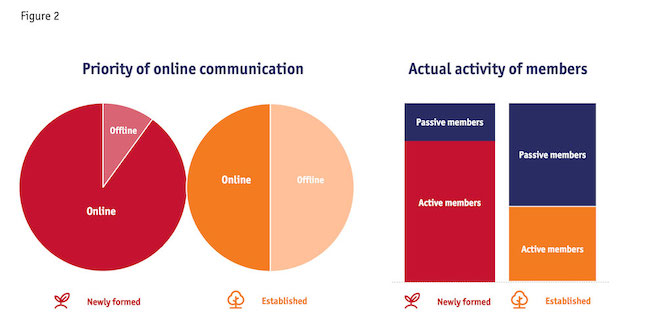 Newly formed communities do not have physical representatives in the regions, but since they are online communities, they cover almost the whole territory of their country and include parents from remote regions that cannot be part of established communities due to lack of representation in those regions. So, our first observation is that these communities – even without regional representatives – have bigger coverage of caregivers who actively communicate in their WhatsApp and Facebook groups daily (Figure 2).
Newly formed communities do not have physical representatives in the regions, but since they are online communities, they cover almost the whole territory of their country and include parents from remote regions that cannot be part of established communities due to lack of representation in those regions. So, our first observation is that these communities – even without regional representatives – have bigger coverage of caregivers who actively communicate in their WhatsApp and Facebook groups daily (Figure 2).
Local changes
We’ve witnessed that newly formed communities are pragmatic self-help circles that caregivers organize to help each other rather than bring about some significant changes on the national level. This is the core of their value system, which makes them flexible and agile. They stand for local changes and helping individuals rather than focusing on systemic changes in the health care system. This will be our starting point in understanding what value this type of community can bring to health care research. These communities accumulate a big amount of educational information and even medical expertise. As we saw in Russian newly formed communities, these PCs often consider themselves experts alongside professional health care providers who, in the case of rare genetic diseases, happen to be even less informed than the caregivers. PCs keep track of all the latest news on drugs and results of clinical trials, they study the treatment and rehabilitation process in detail and they have deep knowledge of medical equipment, drugs and the actual situation with the supply of subsidized drugs.
 Another important type of data that newly formed communities accumulate is the life of the community itself. This includes caregivers’ and patients’ experience, the ways they help and support each other and their knowledge of government and pharma programs and opportunities.
Another important type of data that newly formed communities accumulate is the life of the community itself. This includes caregivers’ and patients’ experience, the ways they help and support each other and their knowledge of government and pharma programs and opportunities.
Observed common features
To gain a multicultural understanding of PCs for our research, we approached DMD patient organizations in the three countries. We had different experiences of recruitment in each of these three regions but we also observed common features of recruitment of newly formed communities across the countries.
 We tried to contact established PCs in the U.S. using their official contact details available on their websites. However, we couldn’t reach them. The main reason was that those organizations are quite large and tended to ignore our calls and e-mails – or a gatekeeper referred us to another person and we could not find the right person to talk to. Another issue was related to the restrictions on the public usage of information we could gather. Many groups in the U.S. were required to sign official papers prohibiting the sharing of any data outside the organizations. Obviously, we could not conduct our interviews under these conditions. Having failed to contact the established communities through the official channels, we tried to reach them via their groups on Facebook. That also didn’t work.
We tried to contact established PCs in the U.S. using their official contact details available on their websites. However, we couldn’t reach them. The main reason was that those organizations are quite large and tended to ignore our calls and e-mails – or a gatekeeper referred us to another person and we could not find the right person to talk to. Another issue was related to the restrictions on the public usage of information we could gather. Many groups in the U.S. were required to sign official papers prohibiting the sharing of any data outside the organizations. Obviously, we could not conduct our interviews under these conditions. Having failed to contact the established communities through the official channels, we tried to reach them via their groups on Facebook. That also didn’t work.
The situation with established communities in the countries where we had personal contacts with them was different. We worked before with Parent Project Russia, so they were eager to participate in our research and they gave us contacts and recommended us to other Russian patient communities. Due to the small size of the Russian DMD community and personal connections between all activists, we easily got in touch with all of them. The Indian community was also easy to get in touch with. They responded immediately without any personal contacts and were eager to participate.
After we failed to recruit established communities in the U.S., we turned to help from an organization that acts as an intermediary between patients/caregivers and pharma – the Rare Advocacy Movement (RAM). This organization protects the rights and interests of patient communities and its core consists of newly formed independent groups of caregivers. During our recruitment journey, we discovered that most of those communities do not have professional lawyers, so they delegate the advocacy function to an intermediary such as RAM.
As soon as we started working with RAM, we found out there are many small online parent organizations in different states whose main goals are fundraising and targeted help. The newly formed PCs in the U.S. are rarely institutionalized but quite effective with the support they can give to their members. Still, without the support of an advocate like RAM, these communities are often invisible and hard to reach. And even if we could find some of them without the help of RAM, they were not open to participate in our research. Without the connection of an intermediary like RAM, the PCs were not inclined to trust us and see the benefits of collaborating with a research firm. We ran into the same conundrum in Russia with a newly formed community called Gordey. Based on our findings, intermediary advocacy organizations such as RAM play a crucial role in the recruitment of the newly formed communities.
Even deeper insights
Our research provided us a great depth of knowledge of patient communities, which can offer other researchers even deeper insights into how to work with these types of communities and other difficult-to-reach or niche online communities in the future.
If you know how to communicate with specialized communities, they open more opportunities and insights for research. Without having the proper tools, these communities are almost invisible. But with the right tools, these communities can shed a great deal of light and offer new perspectives and insights that market researchers might not typically have access to.
5 key takeaways from working with patient communities
1. We identified a particular type of patient community that we termed newly formed that values flexibility, online presence and independence from pharma companies. This type of community covers a larger audience of caregivers who are more pragmatic than ideological – they do not invest their time fighting for patients’ rights; rather, they help each other solve specific issues, such as fundraising and providing educational support.
2. The advocacy function is not developed in newly formed communities. So, in order to get in touch with these communities, be ready to communicate with parents using the professional assistance of intermediary advocacy groups.
3. As these communities initially are not set up to receive financial support from pharmaceutical companies and the government, they are interested in non-profit collaborations as well as informational and educational support.
4. Their initial focus is on finding reliable information, so newly formed PCs are thirsty for firsthand knowledge of drug innovations and clinical trials.
5. Some of the newly formed communities are concerned about their reputation as experts. They are interested in scientific publications where they are given proper credit and in having an advisory role in the development of new drugs.