Editor's note: Lynn Welsh is chief strategy officer, and Amanda Lipski is director, research services, at Olson Research Group Inc., Yardley, Pa.
The U.S. health care system is expected to spend more than $150 billion treating cancer by the year 2020. Compounding this, of the 20 orphan drugs expected to reach blockbuster status by 2018 (+$1 billion in sales), 13 are oncologic agents. It is not surprising that the increased number and cost of new oncology therapies has translated into a greater prevalence of marketing research conducted across the broad spectrum of oncology therapies in the past few years. At our firm, Olson Research, we see this evidenced in the sheer number of projects we have undertaken in this therapy area: in the last 18 months alone we have fielded over 300 research studies in oncology. The focus of this article is one such study, which was designed to uncover oncologists’ perceptions of a new incentive program introduced by health insurer WellPoint Inc.
Signaled a shift
The last several years have signaled a shift in how payer organizations are attempting to control the escalating costs associated with treating cancer. A significant rise in both the number and cost of targeted therapies has led payers to initiate programs that encourage oncologists to adhere to standardized treatment guidelines. The trend has been to incent oncologists who comply with the treatment protocols established by payers for various cancers.
In July 2014, WellPoint – which changed its name to Anthem Inc. in December 2014 – began offering oncologists a monetary incentive for each patient who receives treatment for breast, colorectal and lung cancer, as specified by one of the insurer’s recommended regimens. Oncologists would receive a one-time $350 payment at the onset of treatment planning and care coordination. The practice would also receive $350 per month per patient while the patient was active in therapy and on one of the recommended pathways. This approach by payers to more greatly influence oncologist prescribing choices by incentivizing physicians to choose certain treatment approaches had the potential to be a very polarizing and provocative subject in the oncology community.
Beyond the cost savings it may afford payers, standardizing treatment pathways has the potential to create efficiencies in patient care. Yet, we are living in a time of great improvements in targeted cancer therapies and these are expanding the boundaries of individualized approaches to treatment. How would WellPoint’s incentive program affect physicians’ and patients’ desire for personalized treatment approaches? How, if at all, would WellPoint’s standardized treatment pathways integrate new, innovative advances in medicine? WellPoint’s program raised a multitude of issues, including the question of who should be determining treatment: payers or physicians?

Determine the best methodology
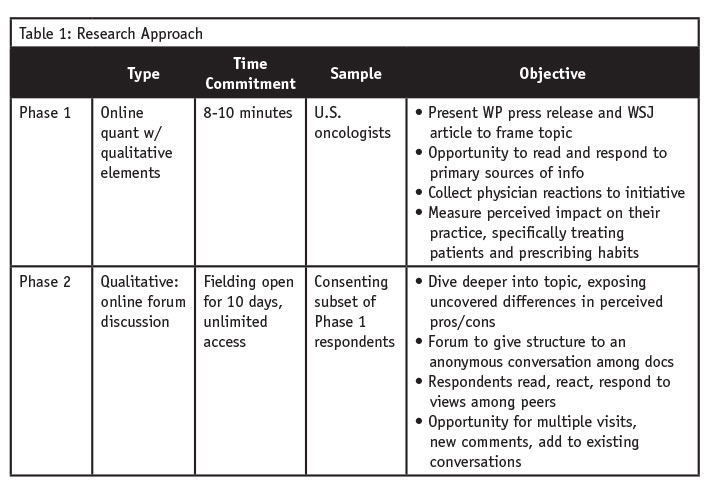
We first had to determine the best methodology to evaluate perceptions of such a highly provocative issue. To start, we wanted to measure awareness and understanding among oncologists of the WellPoint program and to gauge their reaction upon reviewing primary source information on the program and its intentions. For this, we needed quantitative measurement. As outlined in Table 1, we elected to field an eight-to-10-minute online quantitative survey with U.S. oncologists to measure awareness of the program and gather opinions on how the program might affect their practice and prescribing habits. From within the survey, physicians were asked to review two primary sources on the WellPoint program: the WellPoint press release announcing the implementation of the Care Cancer Quality Program and a Wall Street Journal article (“Insurers push to rein in spending on cancer care,” May 27, 2014) describing the initiative.
Beyond measuring awareness and knowledge, as the topic was explored further, we were aware that the debate surrounding the implications of the WellPoint program would elicit differing opinions. We also knew that opinions could be highly personal and rooted in larger issues of physician reimbursement and prescribing autonomy. We felt that the perceived effects of WellPoint’s program could be most fully explored by generating interaction between oncologists and we predicted that discussions may become somewhat charged.
In a face-to-face setting, we knew that there was the very real possibility of a physician pecking order emerging, where veteran, more experienced physicians, or perhaps those designated as key opinion leaders in their particular field of oncology practice, might heavily influence the tone and direction of a live conversation. More practically, physicians are also busy professionals for which in-person research participation is not often feasible. For these reasons, we felt an online forum discussion would be most appropriate.
At the conclusion of the survey, respondents were asked to consent to a further online discussion forum a few days later to more deeply explore the effect of the WellPoint program on both physician practices and patient care. The online discussion forum allowed us to capitalize on the richness of the comments from the qualitative elements in our survey. We took the prevailing arguments uncovered in the first research phase, those both for and against incentive programs such as WellPoint’s, and turned them into discussion topics for the online forum.
Engaged and interested
The first phase of the research project was fielded in two weeks. Responses were on-point and thorough; physicians were engaged and interested in the topic. Oncologists spent an average of eight minutes on the survey. The hybrid quant/qual approach of the survey successfully allowed us to measure awareness and understanding of the WellPoint program, while at the same time posing quite a few open-ended questions, allowing us to fully ascertain reactions to the WellPoint program.
Despite the strong opinions voiced by the oncologists who participated in our survey, only 32 percent indicated that the incentive program might change or alter their behavior. Many suggested that they were likely to adhere to the treatment pathways recommended in the future. See Figure 1 for detailed comments directly from our research.
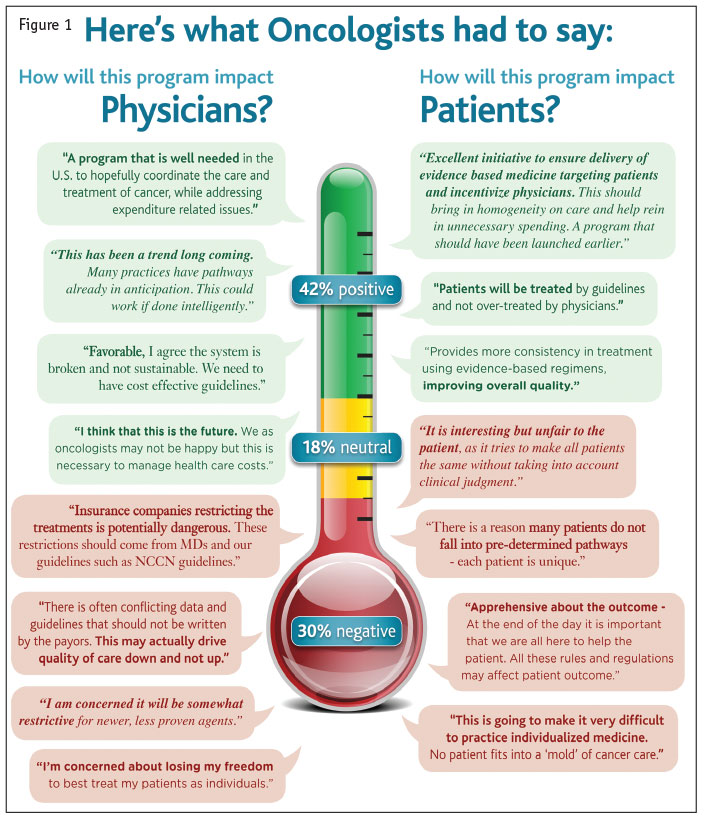
Those in favor of the program expressed optimism that the program would dissuade unnecessary excessive treatments and also help to give oncologists some much-needed guidelines or boundaries within which to care for their patients. Some also opined that personalized medicine can offer patients false hope and that it is better to set expectations based on what medically-proven therapies can deliver.
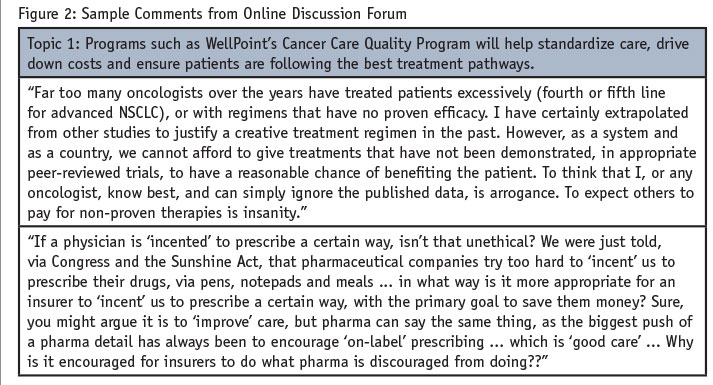
It was evident that the forum approach was the right methodology to use for this population. Participation was frequent and regular, comments thoughtful, discussions lively, and a few heated debates ensued. (See Figure 2.)
Deliver a robust outcome
Three underlying factors contributed to the success of this research. First, having a recognized and trusted relationship with your target market facilitates strong participation. Second, while not always under our control, timely topics or subject matter can assist in fielding success. Lastly, and perhaps most important, spending time at the project outset to ensure your methodology is most appropriate for the research need can deliver a robust outcome.
We recognize that a quantitative-first, qualitative-second approach is not the customary sequence to marketing research and that there are sound methodological reasons for pursuing a more traditional trajectory in most cases. However, the success of this project supports the basic premise that researchers should employ the methodology and tactics that will best deliver results. Making a sound decision to align the research methodology with your target population, time frame and subject matter can ensure successful data collection – a vital element for delivering sound results to clients.