Editor’s note: Lucio Corsaro is general manager at market research firm MediPragma, Italy.
This post was inspired by a Quirk’s e-newsletter article, “How will consumption change in post-coronavirus China?” published on February 24, 2020. In this post, I will share a market research perspective on the impact of the coronavirus in Italy. In particular, this project aims to develop observations and hypotheses on new operational and patient management models that may arise after the development of the infectious outbreak in our country.
The coronavirus outbreak will dissolve eventually. After the storm, what will happen to the current medical-patient communication and working models? I have tried to answer to the questions of the original article but in a completely Italian context and more specifically from the outpatient physician's perspective.
1. Will the coronavirus epidemic shift or create a new working environment for the Italian outpatient doctor?
Physicians are not enthusiastic about all the demands coming from patients right now or about using tools such as phones, WhatsApp or social networks, because they do not feel adequately prepared and trained to manage the visit using remote tools. A variety of challenges exist for remote visits, such as drawing up illness certificates on the basis of medical history collected by telephone, without being able to see the patient in any way – not to mention the security and data privacy issues presented by online health care.
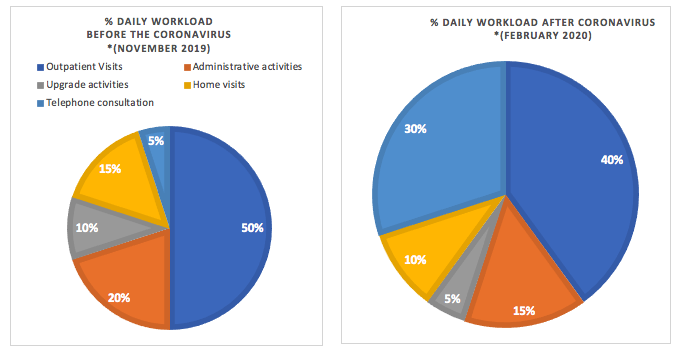
Beginning early this month, the workload of the outpatient doctor has changed. The physician does not receive people in the office, but the patient remains in the waiting room and describes their symptoms to the physician. Then, the doctor with the mask communicates that, at the moment, he does not visit patients. In regions affected by the virus, there are virtually no home visits in favor of electronic receiving and teleconsultation. The scientific information of companies has also suffered a setback with the suspension of all activities of the external network in the areas affected by quarantine measures; the suspension of all national and international transfers of headquarters staff; and the request to carry out activities remotely.

*Continuous CATI/CAWI MediPragma survey with 200 general practitioners and 100 pediatricians of free choice.
The question is whether this could persist, with different percentages, even after the end of this emergency period. The answer is that there will most likely be a slow return to normality – to the habits that doctors had before, as well as medical and scientific information from external company networks – with some organizational consequences.
So, how will the habits of outpatient doctors change after the coronavirus? Among the experts consulted, it is thought that: "The changes in the physician's work will be achieved if this situation persists over time, but if, as we hope, it is limited to a few days, I do not think it will have a lasting effect on his work.” The answer to this question could encourage companies to also use digital tools also to support doctor training.
2. Will the coronavirus epidemic give rise to a new business model?
Prior to the coronavirus epidemic, the online search for health-related information was already among the most-clicked topics and pharmaceutical e-commerce was growing due to the online purchase of supplements and over-the-counter medications. However, after the coronavirus epidemic, we could observe many online activities flourishing, such as an acceleration of telemedicine/teleconsulting and, at the same time, an increase in drug home deliveries (including red prescription – the official document that shows you are doing a procedure within the Italian national health care service).
Also, the use of remote scientific information systems by reps and external sales forces (e.g., medical scientific liaison, key account manager, etc.) may be the subject of greater development. The point will not be the technology already available, but a change of working mind-set of these professionals. Therefore it will be necessary to expand their training to develop the necessary skills to conduct remote interviews.
The coronavirus epidemic will certainly cause a major blow to the economy, but what new business models might it promote? Remote working was on the rise prior to the coronavirus and will probably increase in popularity. The tools and methods that facilitate remote working may become more sophisticated and employees who have now experienced the convenience and efficiency that comes with remote working may grow more inclined and accustomed to it.
Other hypotheses on the effect of the coronavirus on potential new business models include:
- The current risks for the distribution system, in particular for pharmacies, could increase the popularity of online pharmacies and home delivery with a possible acceleration toward the use of drones.
- Local health authorities (LHA) could be equipped with more staff for door-to-door services, or light garrisons in the territory (An opportunity to enhance the value of the pharmacy services?), to relieve the congestion of both the emergency rooms of hospitals and the medical offices themselves. Local health authorities could be equipped with more staff for door-to-door services, or light garrisonsin the territory, to relieve the congestion of both the emergency rooms of hospitals and the medical offices themselves.
- Strengthening of telediagnostic, teleconsultation and telemedicine tools with an increase in security and privacy issues between physician and patient.
- The training and educational offers could be oriented more and more toward updating events and exchange of opinions. Distance medical training (also through 3D simulation) will push institutions and other providers to reconsider the offer and the training channels. An example of this is given by Fnomceo (national federation of orders of surgeons and dentists) with the first FAD (distance learning) course with information updated in real time.
- The role of reps will remain crucial and the visit for scientific medical information will never be completely replaced by technology, but it will accelerate the path of digital transformation that many companies are already implementing. "COVID could leave a greater rigidity in accepting the entry of the reps in different health facilities (mainly hospitals and LHA), with dramatic consequences in terms of employment. All of these visits would also be poured and clogged up in the GPs and private sector. Of course, the idea of developing more a remote reps that can interact digitally with its doctors, is a totally new model to build and that could occupy a part of smart working."
In the same way that SARS sparked a rapid development of e-commerce in China and the Great Hanshin earthquake ushered a collaborative consumption norm into Japan, the coronavirus epidemic, along with the 5G technology, will catalyze the prevalence of new business models (see "The Rise of Sharing: Fourth-Stage Consumer Society in Japan" by Atsushi Miura).
3. How can the mentality and behavior of outpatient doctors and other medical categories be influenced by the coronavirus epidemic?
The crucial element to answer this question is time! It is important to make a reflection on some aspects: the change of mentality and behavior will be directly proportional to the duration of the emergency. "The longer this emergency will last (hopefully the least possible) and the more marked will be the change of mentality and behavior."
The physician's approach could change in four areas: the relationship with institutions (in this case also employers); uncertainty about diagnosis and therapeutic decision; information asymmetry (given also, but not only, by social networks); and the impact of factors external to the disease (e.g., cultural factors).
Regarding the relationship with the institutions, clinicians share the view that, "Today the coronavirus leads us to consult institutional sources to orient us among the various procedures to be undertaken. The electronic tool is indispensable to standardize physicians' behaviors. This can be applied to other fields. Once the storm has passed..." In this context, medical associations and the scientific societies will be able to develop further protocols of remote examination for many pathologies.
The uncertainties and the asymmetrical information that it has generated on the web and social networks will trigger a return of confidence on the physician's work (in spite of Dr. Google) but the physician will have to be able to exploit this return of trust to regain a role that they partially lost through a new way of updating (more timely and more digital) and to communicate even at a distance with patients or groups of patients through the use of assertiveness and empathic communication techniques, adapting it to four different clusters: older populations, working populations, Millennials and populations with rare and/or chronic diseases.