
The heart of the matter
Editor's note: Tom Donnelly is chair of the Intellus clear health communication task force. He can be reached at tom.donnelly.phd@gmail.com. Barbara Haimowitz is president of the DataMine Inc. She can be reached at barbanalysis1@gmail.com. Tatiana Barakshina is managing partner at Bazis Americas. She can be reached at tvb@bazisgroup.com. Kinshuk Sahni is data analyst at Compoundexpress. He can be reached at kinshuk.sahni6@gmail.com. Heaven Russell is healthcare public relations coordinator at Bazis Americas. She can be reached at h_russell@bazisgroup.com. The authors would like to thank Sago for its project management and health care provider recruitment assistance. This project was funded by Intellus Worldwide, a not-for-profit organization dedicated to advancing the field of health care insights and analytics.
Clear health communications are critical in the emergency room (ER) setting, in which timely treatment can potentially make a lifesaving difference. Any delay in treatment could lead to adverse health outcomes, morbidity and mortality.
Treatment is initiated based on correct triaging, an in-depth clinical understanding of symptoms, an evaluation of lab values and other measurements and the patient’s overall disease presentation. This process from triaging to treatment is driven to a great degree by doctor-patient communications and the mutual interpretation of these interactions. An optimal ER treatment and follow-up necessitates that the patient and their provider understand each other, in all circumstances, either directly or through translation, regardless of health literacy level.
In a previous study,1 we found that doctors and other health care providers (HCPs) are often inaccurate in identifying the health literacy levels of their patients, especially in patients with limited English proficiency (LEP), prompting the need for simple explanations to be used with all the patients, regardless of their health literacy status.
High levels of clarity needed
We began to think about treating LEP patients and considered where communication between patients and HCPs needed high levels of clarity, singling out the ER as the place where clear health communication is critical. To narrow our research more, we asked the HCPs about their experiences with cardiovascular disease (CVD) patients. Patients with coronary artery disease, ischemic heart disease or a history of myocardial infarction account for 6.4% of ER visits indicated on the medical records. CVD events are scary, can occur out of nowhere, create emotional upheaval and sometimes require immediate treatment to save lives.
There are many negative outcomes due to language barriers2 in general and these issues are applicable to approximately 8.6% of the U.S. population, classified as people with LEP: larger surgery delays; fewer health screenings; higher central line infections; more falls; less-accessible health care; longer stays in the hospital; and more medication management issues.
With an objective to minimize or completely avoid these negative outcomes, we wondered:
- How can language differences be overcome?
- How long does it take to get help if a language gap exists?
- What aspects of the process are most challenging during an ER visit?
- What strategies do HCPs use to ensure the dialogue with the patient goes smoothly?
In this study we have looked at several meaningful ways to segment participants to achieve deeper insight in the communication needs and challenges with LEP patients.
- Specialty: Doctors vs. nurses
- HCPs from low-, medium- and high-resource areas – defined by a U.S. county’s percent of people lower than federal poverty level (%FPL)
- HCPs with patients who have limited English proficiency (HCPs with <60% or >60% patients whose primary language is English)
Sample and methods
We conducted a 15-minute online survey with n=93 emergency department HCPs. The study was executed with the support of Sago. Fifty-eight percent of the HCP survey participants were male and 42% were female. The emergency department MDs had an average of 17 years in practice, while the emergency department nurses or certified emergency nurses had an average work experience of 12 years. Additionally, MDs typically saw an average of 376 patients in the ER every month, whereas nurses saw an average of 242 patients. We achieved representation of each of the three geographic segments – low-resource (n=15), medium-resource (n=45) and high-resource (n=33) areas – although getting participants from the low-resource area was particularly challenging due to a lower representation of physicians from these areas in the traditional research panels. Thirty-nine percent of providers were classified as “low-English-proficiency barrier” segment (since they work with >60% of patients with English as their primary language), while the remaining 61% of providers fell into “high-English-proficiency-barrier” segment, with <_60% of their patients fluent in English.
Results
Our research revealed a number of intriguing and potentially impactful findings. On average, it takes about 11 minutes until language assistance arrives for LEP patients. The wait time increases to almost 45 minutes in low-resource areas. Imagine what this wait time means for a cardiovascular patient in need of immediate help.
HCPs say that the topics that are most difficult to understand for LEP patients are how to reduce stress and how and when to take medications. Nurses echo this finding, stating that LEP patients find it somewhat to very difficult to understand how and when to take medications. The nurses mentioned medication management significantly more than the MDs because they are directly involved in ensuring that the patients stay adherent. The nurses are also instrumental in the discharge instructions.
Similar trends are also seen among HCPs treating high-language-barrier patients. About half of all HCPs use a virtual interpreter. More MDs use them than nurses and one-third use a wearable HIPAA-compliant device.
To aid our mission to bring increased awareness of health literacy among HCPs, we created a summary of clear health communication techniques that physicians and nurses can use both inside and outside of the ER. We came up with three categories to organize these techniques into: verbal, nonverbal and aids and materials (Figure 1). Our team feels passionately about a few of these techniques, including using plain language when explaining things to patients and using everyday examples to illustrate a medical term.
![]()
Clear health communication techniques
In our study, nurses indicated a significantly higher use of clear communication techniques (compared to physicians), including the use of plain language, to ensure that their CVD patients understand their instructions. Physicians, on the other hand, are more reserved when it comes to self-reporting the use of these techniques. MDs use them when the situation calls for them or only occasionally. Very few MDs are mindful of body language, position and eye contact as ancillary drivers of achieving clear communication goals with their patients.
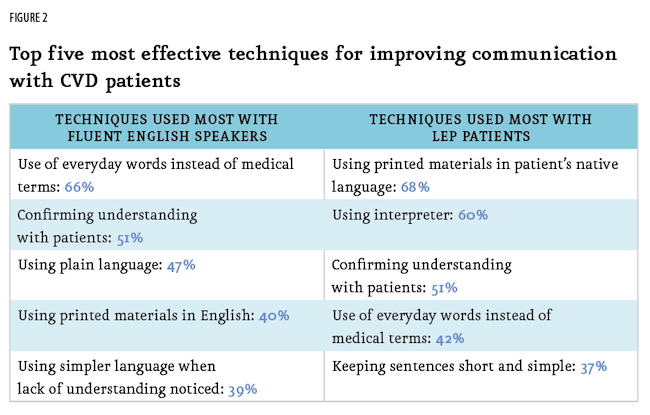
We observed, as noted in Figure 2, significant differences in the techniques providers find effective when working with patients fluent in English compared to those with LEP. For instance, with LEP patients, HCPs frequently use printed materials, conduct frequent check-ins to confirm understanding and simplify sentences by keeping them short. In contrast, techniques such as using everyday words instead of medical terms and confirming patients’ understanding are applied more consistently to all patients, regardless of language proficiency.
Our study revealed a notable gap in the application of shared decision-making (SDM) principles – a collaborative process in which patients and health care providers jointly make decisions, considering the best-available evidence alongside the patient’s values and preferences.3 These principles are more frequently deployed with English-proficient patients compared to those with LEP. We identified three key areas in which the SDM gap exists between these groups (according to providers’ self-report of the application of these techniques). The following techniques are applied less frequently by providers while consulting patients with LEP: assessing patient preferences regarding treatment; incorporating patient preferences into the discussion; and explaining the rationale behind the proposed treatment to patients. This highlights a potential challenge in ensuring equitable patient-provider exchanges.
Actionable steps
Our research highlights a number of actionable steps to enhance communication with patients with limited English proficiency. Based on feedback from health care providers we identified three key areas for improvement:
First, we confirmed that the availability of timely and accurate interpreter services is crucial. Providers currently rely on live interpreters, video interpreters and translation services but improvements are needed, especially with CVD patients in the ER. Increasing the availability of interpreters, expanding video-interpreter services and ensuring interpreters are easily accessible – whether in person or virtually – can significantly reduce waiting times. This improvement would establish a basis for more meaningful and effective interactions between providers and LEP patients.
Second, building awareness among ER providers about effective patient engagement strategies is essential. These engagement strategies include using plain language, spending additional time with patients, involving family members in discussions and ensuring follow-up care, thereby increasing the likelihood of treatment and medication adherence. Repeated explanations and frequent assessments of patient comprehension and asking patients to repeat the HCP’s instructions in their own words are critical to fostering understanding and trust, both for LEP patients and those fluent in English.
Third, strengthening training and educational materials was repeatedly mentioned. For hospital staff, this includes offering training on collaborating with interpreters and hiring more bilingual or multilingual staff. For patients, particularly in areas with high LEP populations, providing educational materials such as videos, handouts and written resources in multiple languages can help explain disease processes, treatment options and care expectations. This is especially important as patients transition to their community HCP after discharge from the ER.
These initiatives can bridge communication gaps and improve care outcomes for LEP patients.
A note on sampling in the low-resource areas: While conducting this research, it was challenging to recruit in counties with a high percentage of population below the federal poverty level (the segment we referred to as “low-resource area” in this study). This happened specifically in states such as South Dakota, Mississippi, Louisiana and Alabama. HCPs in low-resource areas are hard to contact and often don’t participate in research studies. Web panels don’t always reach into these underserved areas. Social determinants of health/health inequity factors also pose significant concerns. It is important that we, as market researchers, get an unbiased handle on health literacy around the entire country, not just in the bicoastal areas and the Midwest. Physicians and patients in low-resource areas grapple with unique issues and deserve to be included in marketing research. We need to establish match rates for high-/medium-/low-resource areas. It will be important to work with the American Medical Association, which supplies NPI information to its selected vendors.
Learnings emerged
From a research planning and implementation perspective, several important learnings emerged.
- When conducting quantitative health care research with patients or providers, it is essential to ensure representation from populations with low health literacy and those with limited English proficiency.
- Adopt a mixed-method recruitment strategy to effectively reach low-resource areas. Collaborate proactively with panel providers to identify potential gaps, set realistic client expectations and build in an additional two to three weeks to ensure adequate representation.
- Finally, consider potential differences in communication strategies between physicians and nurses when interacting with patients, as these may influence research findings.
References
1 Donnelly, T., Barakshina, T., Kirk, J., Stone, B. and Ashley-Collins, H. (Sept. 2020). “Clearly better: Study underlines the importance of clarity in doctor-patient communication.” Quirk’s Marketing Research Review.
2 Agency for Healthcare Research and Quality. (n.d.). “A Patient-Centered Guide to Implementing Language Access Services in Healthcare Organizations” (Publication No. 10-0046-EF). U.S. Department of Health and Human Services. Retrieved from https://www.ahrq.gov/sites/default/files/publications/files/lepguide.pdf
3 Kanzaria, Hemal K., Robert H. Brook, Marc A. Probst, Dustin Harris, Sandra H. Berry and Jerome R. Hoffman. “Emergency physician perceptions of shared decision-making.” Academic Emergency Medicine 22, no. 4 (2015): 399-405.